A little-known federal contractor is a big player in privatizing government services
We are again discussing people on Medicaid who may not know they have to reenroll. The largest unknowing segment of that population are those over 65 years of age. This is a combination of several different articles on the Medicaid Disenrollment occurring today. Private business again taking advantage of the lack of knowledge of people and the situation.
The Company Salivating Over The Medicaid Disaster (levernews.com), Matthew Cunningham-Cook
Daniel Hatcher, a law professor at the University of Baltimore who has studied Maximus.
“One of the big concerns is Maximus, a company really making money coming and going from county, state, and the federal governments. People benefiting the most are the company and occasionally governments, but not the people who are supposed to be benefiting from Medicaid services.”
Along with draining public finances, Maximus and other Medicaid redetermination contractors are incentivized to advocate for making Medicaid even more of a bureaucratic nightmare for recipients.
“If you look at the payment structure of these contracts, the more red tape made, the more money Maximus makes. The harder it is to get enrolled, the easier to get kicked off, and again the more money Maximus and contractors are making.”
Maximizing Profits
During the COVID-19 pandemic, lawmakers required states to stop removing people from Medicaid. Which every person knows is the national health insurance program for low-income Americans. The move led to record enrollment in a strictly means-tested program. A program designed to benefit only the very poor. Also a program from which people are often arbitrarily removed.
Late last year, Congress passed a bill of discontinuance and President Joe Biden signed a year-end spending bill directing states to resume annual redeterminations of Medicaid recipients’ eligibility for the program. Now, an estimated 17 million people, and potentially up to 24 million, face the prospect of losing coverage.
As I reported here, nearly half of Medicaid enrollees being disenrolled had not been through a Medicaid renewal process in the past. They were “that” new to the process. Included in this administrative snafu are the “two-thirds (68%) of Medicaid enrollees who are 65 and older and the more than half of Medicaid enrollees who are between the ages of 18 and 29 (53%).”
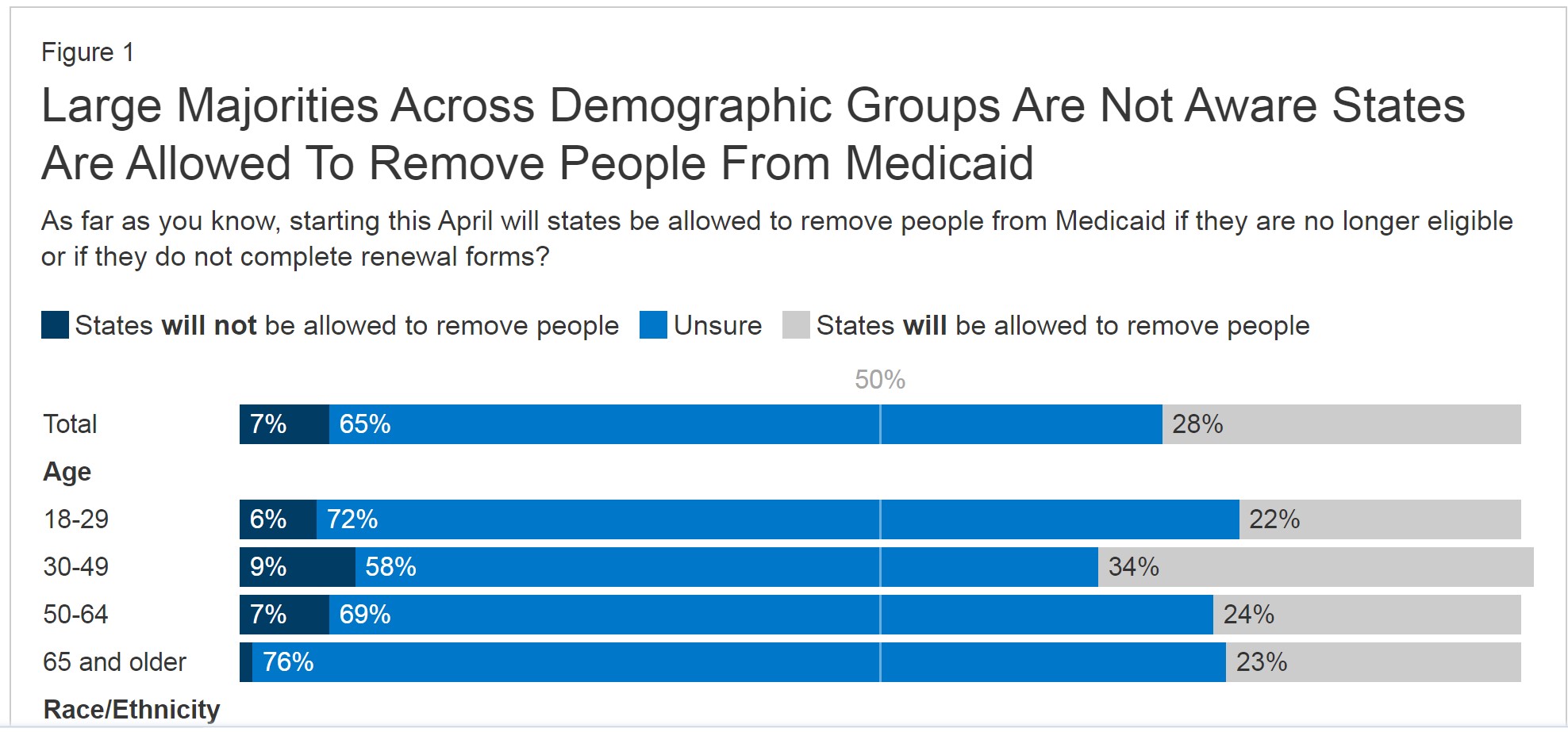
Source: KFF Survey of Health Insurance Consumers (Feb. 21-Mar. 14, 2023)
It has been determined, the expansion of Medicaid coverage reduces deaths, and also has a positive impact on people in poverty throughout their entire lives.
So as KFF determines the numbers of people not knowing they need to enroll again, the job for Maximus became far easier. Easy pickings if they do not reenroll.
While there are significant reporting gaps as to where Maximus is doing redeterminations and how states are reporting eligibility reviews, Maximus still dominates 60 percent of the Medicaid eligibility market, according to a recent report in Modern Healthcare.
While the final determinations for Medicaid eligibility must be completed by public employees, every other step of the process, from processing applications, to running call centers, to reaching out to people on the verge of losing benefits is done by private contractors.
In a recent investor presentation, Maximus wrote that it was boosting its “revenue and earnings guidance to account for Medicaid redeterminations,” and noted that “actual volume flow and beneficiary interaction will influence overall profitability.”
So far, more than 70 percent of those who have recently lost Medicaid coverage have been terminated for administrative reasons, such as not responding to a piece of mail or getting dropped from a call with a redetermination specialist, rather than because they were deemed ineligible due to their income and assets. Many of these people are likely still technically eligible for the program.
Maximus runs the call center for Medicaid eligibility in Indiana, where 85 percent of the 107,000 people kicked off Medicaid this year lost coverage because of procedural reasons. According to Maximus’ $400 million Indiana contract, up to seven percent of its eligibility calls in the state in a given week can be dropped before the company is penalized.
Maximus said in a statement to The Lever . . .
“We do not make Medicaid eligibility determinations. Our job is to support the states’ responsibilities to ensure that everyone who is eligible for Medicaid remains covered. If they are no longer eligible for Medicaid, we work with the states to refer them to other healthcare options such as the insurance marketplace. We are not paid in any state on the basis of whether an individual is found eligible or ineligible.”
Maximus did not answer follow-up questions about the scope of its work in various states and how much revenue the company expects to generate from its Medicaid redetermination business.
As Maximus seeks to expand its Medicaid redetermination work, the company has leaned into lobbying and political donations.
Maximus has donated $2.5 million to national political groups affiliated with state and local politicians since 2017. This includes $955,000 to the Republican Governors Association; $665,000 to the Democratic Governors Association; $450,000 to the Republican State Leadership Committee, which funnels money to GOP state legislative campaigns; $210,000 to the Republican Attorneys General Association; and $165,000 to the Democratic Attorneys General Association.
The company also donates to the National Governors Association, a nonpartisan group that represents governors from both parties.
Maximus spent $960,000 on federal lobbying alone in 2022, and its roster of lobbyists included former longtime Rep. Al Wynn (D-Md.). Wynn is now a senior director at the lobbying powerhouse Greenberg Traurig.
Wynn also was one of just a handful of members of the Congressional Black Caucus to vote “yes” on the final vote on the 1996 welfare reform bill. The legislation, which led to a doubling of extreme poverty, provided an enormous boon to Maximus by incentivizing the outsourcing of welfare eligibility work.
Shar Habibi, the research director of In The Public Interest, which advocates against privatization, said that Maximus’ role in Medicaid redeterminations will hollow out the government’s ability to effectively provide public services. She asked.
“When governments contract with firms like Maximus to do essential public functions like determining who is or isn’t eligible for Medicaid, the question gets raised:
Does outsourcing eligibility determination-related functions compromise the integrity of the program, especially when people’s lives are at stake? Using contractor staff does not promote an effective, efficient, and equitable delivery of Medicaid.”
Maximus also has major contracts with the federal government to provide assistance to those seeking to enroll in Medicare, the government health insurance program for seniors and those with disabilities, as well as those looking to sign up for individual health insurance plans offered on state marketplace exchanges created under Democrats’ 2010 health care law, the Affordable Care Act.
Some people formerly on Medicaid will move to exchange-based plans, which will almost certainly result in substantially higher out-of-pocket costs.
In May, Maximus laid off 700 workers from its Medicare and marketplace call centers where workers were seeking to unionize with the Communications Workers of America (CWA) union. The move led CWA to file an unfair labor practice charge with the National Labor Relations Board and launch a petition to pressure Secretary of Health and Human Services Xavier Becerra to investigate Maximus’ labor practices.
Meanwhile, Maximus’ government contracts to do such work have continued to expand under the Biden administration, despite the fact that Joe Biden pledged in his 2020 campaign that “I intend to be the most pro-union president leading the most pro-union administration in American history.” In September 2022, Maximus was awarded a $6.6 billion contract from the Center for Medicare and Medicaid Services (CMS) in September 2022.
Samira Burns, a spokesperson for the Health and Human Services Department (HHS), which includes CMS, told The Lever the department has initiated a request for information process with contractors like Maximus “to seek recommendations and remain in alignment with industry best practices to ensure we continue to meet national program missions and strategies. In recent years, there has been increasing labor concerns at certain call center locations. HHS/CMS is looking to explore ways to prevent or mitigate ongoing and future concerns.”
I just got a feeling that regardless of their compensation structure, in some places contractors will “guess” that state “A” is okay with more enrollment rejections.
Eric:
States are typically understaffed. They should be recruiting people into these programs as it is cheaper to treat an insured person than one uninsured. This holds true for people on Medicaid or Medicare or CHIPs or any combination such as Medicare and Medicaid.
If understaffed, states still have the responsibility of laying the ground rules and also reviewing the actions of the vendors doing the surveys. Why should taxpayers pay for people unjustly kicked off the programs (which I did supply a reason for this occurring) . The vendor assumes the state will never check or follow up on the discontinuance. These people had a right to be on Medicaid and deserved to be helped instead of punished due to innate grudges.
looks like the medicine industry congress complex is learning to “pick up” admin and advisory services like those contractors shadowing government offices in the dod.
they can charge for hours, and send the contract officers activity reports, bureaucracy on contract
Paddy:
That is exactly right.
I am not sure where you live. I can only guess. We make enough mistakes when we are not being so deceptive. These people need assitance to get into these programs and stay there as they are less costly than private commercial healthcare.
The US has still not learned it is not a battle with the sole purpose of disenfranchising people or citizens.
https://www.nytimes.com/2023/07/23/us/politics/medicare-drug-price-negotiations-lawsuits.html
July 23, 2023
Drugmakers Are ‘Throwing the Kitchen Sink’ to Halt Medicare Price Negotiations
The government will soon announce the first 10 medications that will be subject to price negotiations with Medicare under a new law. Drugmakers are fighting the measure in court.
By Sheryl Gay Stolberg and Rebecca Robbins
https://www.nytimes.com/2023/07/22/business/gilead-hiv-drug-tenofovir.html
July 22, 2023
How a Drug Maker Profited by Slow-Walking a Promising H.I.V. Therapy
Gilead delayed a new version of a drug, allowing it to extend the patent life of a blockbuster line of medications, internal documents show.
By Rebecca Robbins and Sheryl Gay Stolberg
Sorry. I do not know why a photograph appears now and again in a New York Times post. However, the 2 Times articles are important and germane to the topic.
@ltr,
The topic is medicaid. How is medicare germane to medicaid?
Please do try being polite.
1) Medicaid includes many Medicare recipients.
2) The point is that American healthcare outcomes are significantly worse than outcomes in other high income countries and any healthcare discussion should consider the poor general outcomes.
Thank you for the question.
ltr:
Why are outcomes so bad? Is it because they can not get the healthcare they need, are denied healthcare, are uninsured? Maternity outcomes. With private commercial healthcare, women had access to healthcare after a birth for up to one year. Medicaid did not do such till recently. If you were on Medicaid, you were allowed two months.
I think what you are attempting to say with all the documentation you had posted, much of the issue is the lack of access to healthcare. The entire post is about kicking people who are or could be eligible for healthcare through Medicaid off of it for silly reasons such as not reenrolling.
Not what do they do? Present themselves to a hospital for care under charity care. There are programs for this too. 340B is one of them.
That is your unclarified point, I believe.
Why are American healthcare outcomes so relatively poor?
https://fred.stlouisfed.org/graph/?g=15txV
January 15, 2018
Life Expectancy at Birth for United States, Greece, Italy, Spain and Portugal, 2017-2021
https://fred.stlouisfed.org/graph/?g=15ty3
January 15, 2018
Infant Mortality for United States, Greece, Italy, Spain and Portugal, 2017-2021
Missing Americans: Early death in the United States—1933–2021
May 29, 2023
Missing Americans: Early death in the United States—1933-2021
By Jacob Bor, Andrew C Stokes, Julia Raifman, Atheendar Venkataramani, Mary T Bassett, David Himmelstein and Steffie Woolhandler
Significance Statement
One million US deaths in 2020 and 1.1 million US deaths in 2021 would have been averted if the United States had the mortality rates of other wealthy nations. About half of these missing Americans died before age 65. The number of excess US deaths relative to peers is unprecedented in modern times, at least since the 1930s. These excess US deaths were a result of a decades-long divergence in mortality from other wealthy nations, beginning in the 1980s, and were further exacerbated by the COVID-19 pandemic. The use of an international benchmark highlights unfavorable mortality trends involving all US racial/ethnic groups and disproportionately affecting younger and working-age adults.
Abstract
We assessed how many US deaths would have been averted each year, 1933–2021, if US age-specific mortality rates had equaled the average of 21 other wealthy nations. We refer to these excess US deaths as “missing Americans.” The United States had lower mortality rates than peer countries in the 1930s–1950s and similar mortality in the 1960s and 1970s. Beginning in the 1980s, however, the United States began experiencing a steady increase in the number of missing Americans, reaching 622,534 in 2019 alone. Excess US deaths surged during the COVID-19 pandemic, reaching 1,009,467 in 2020 and 1,090,103 in 2021. Excess US mortality was particularly pronounced for persons under 65 years. In 2020 and 2021, half of all US deaths under 65 years and 90% of the increase in under-65 mortality from 2019 to 2021 would have been avoided if the United States had the mortality rates of its peers. In 2021, there were 26.4 million years of life lost due to excess US mortality relative to peer nations, and 49% of all missing Americans died before age 65. Black and Native Americans made up a disproportionate share of excess US deaths, although the majority of missing Americans were White.
https://fred.stlouisfed.org/graph/?g=14GnX
January 15, 2018
Life Expectancy at Birth for United States, Canada, France, Germany, Italy, Japan and United Kingdom, 2000-2021
https://fred.stlouisfed.org/graph/?g=11RGk
January 30, 2018
Infant Mortality Rate for United States, Canada, France, Germany, Italy, Japan and United Kingdom, 2000-2021
ltr:
This is a healthcare article. Your points are important. The topic is rogue vendors allowed by states to kick people off of Medicaid. If you wish to post an article on those issues, I would help you make a post out of them ltr.
Bill