Medicare Spending Curve Bent
In 2010 Congress passed the Patient Protection and Affordable Care Acts (there were 2) from now on called the ACA. One of the aims was to bend the Medicare spending curve and, they hoped (or dreamed) stop the increase in spending per beneficiary.
The spending per beneficiary ceased increasing.
Oh crap Chrome refuses to upload an image (and says I am offline while also opening other pages. I should have kept my oath). sorry for housekeeping tangent. I am here using Firefox.
Trying again: the spending per beneficiary ceased increasing.
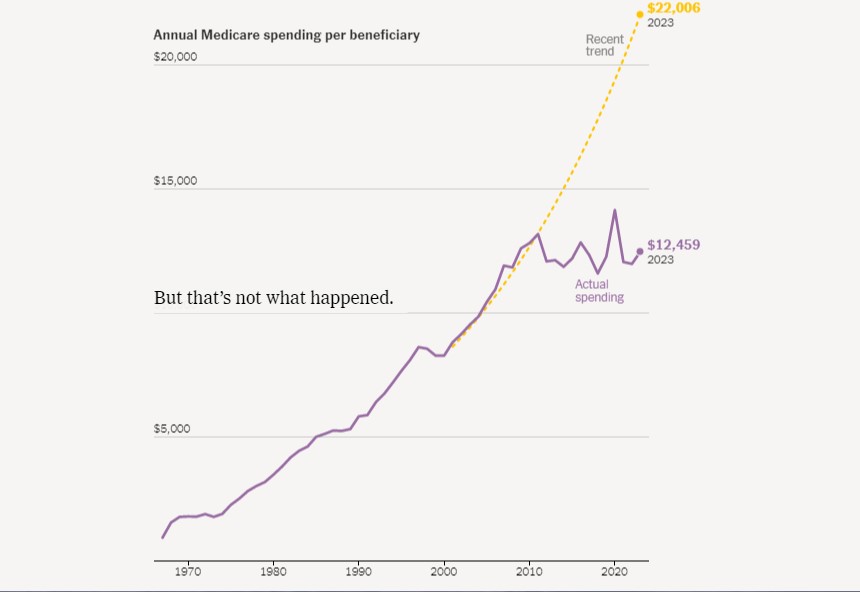
See the very clear dramatic break at 2010. Evidence doesn’t get clearer than that.
In true 200 proof commitment to the tradition that “opinions on shape of planet differ: both sides have a point.”
Margot Sanger-Katz, Alicia Parlapiano and Josh Katz write “The reason for the per-person slowdown is a bit of a mystery.” Yep, probably a coincidence.
Now back in 2010, there were those who asserted that this outcome was unlikely. One was Richard S. Foster of the Centers for Medicare and Medicaid Services. He is quoted and paraphrased by Lori Montgomery questioning whether the ACA cuts to Medicare spending will actually be implemented (by the way the link to the House Ways and Means Committee which should lead to the official document is dead).
“
The report, requested by House Republicans, found that Medicare cuts contained in the health package approved by the House on Nov. 7 are likely to prove so costly to hospitals and nursing homes that they could stop taking Medicare altogether.
Congress could intervene to avoid such an outcome, but “so doing would likely result in significantly smaller actual savings” than is currently projected, according to the analysis by the chief actuary for the agency that administers Medicare and Medicaid. That would wipe out a big chunk of the financing for the health-care reform package, which is projected to cost $1.05 trillion over the next decade.”
I wrote . . .
“I think that ‘Hospitals will refuse Medicare and/or Medicaid’ is a serious policy concern on a level similar to the “tax cuts cause increased revenues.” And here it is on the front page of www.washingtonpost.com.”
I told you so.
FWIW, our local hospital is in the process of “right sizing”, that is shedding any services that lose big bucks. One of the reasons given for the perpetual budget shortfall is the low reimbursement rates for public health programs, including Medicare. IMO it always was more of a glorified ER facility, but it is the only hospital for 40+ miles, and it had been trying to increase their usage for radiology and some of the other equipment.
Rural health care has always been poor.
Hi Jane:
This is pretty recent from February 2023. It has a pretty good take (Urban Institute) on hospital funding as “supported” by local, county, state, and federal funding.Health and Hospital Expenditures
Why Do Rural Hospitals Close? April 2020
Hospital Monopolies Driving Up the Costs of Healthcare October 2022
Small Town and Rural Hospitals Are at Risk of Closing due to Funding June 2023
A Better Way (Potentially) to Fund Rural Hospitals
The last two on this list I believe may provide an answer to your thoughts. Look at the charts. There is another issue. By moving services to more populated areas, some healthcare companies are able to scam the system when they keep the lesser viable hospitals open. I have another post on that issue.
Bill
Hi Robert:
(edited at the end)
Good to have you around. The (your) chart is revealing in terms of totals being spent. There is another way to look at this. And that is the percent of GDP for total healthcare cost.
Also:
Healthcare Costs do not appear to be outstripping the growth in GDP at this time and since 2018. Some more input from a person who I converse with from time to time and not often,
“Sen. Sheldon Whitehouse (D-RI), chairman of the Senate Budget Committee, asked CBO director Phillip Swagel that very question.
Swagel replied in a letter earlier this year that CBO overestimated mandatory spending for health care in the 2010–2020 period by 9%. “Most of the overestimate for the Medicaid and Medicaid programs stemmed from an overestimate of spending per beneficiary, not an overestimate of the number of beneficiaries,” he wrote.
This systematic overestimation of future health care costs by government economists has far-reaching consequences. When CMS gets it wrong, organizational planners around the country are given a faulty notion of how much money will be flowing through the system, which could lead to a misallocation of resources.
When CBO gets it wrong, Congresspersons get a faulty notion of what resources are available to spend on other programs. It also feeds the GOP’s hysteria around balancing the budget, which undermines political support for other social programs, including those that would actually improve the health of the nation.”
Another part of the discussion which fits your scenario is, “what if GDP slows?” We can rest assured the cost of healthcare will not slow. 2020 is a perfect example of the scenario to which I speak and which shops up in both charts displayed. Getting the profit motive of healthcare to decrease is difficult. They are already suing to stop the efforts in Medicare negotiating Pharma pricing.
I attempt to present and write on the issues of healthcare and the costs at Angry Bear. Not always right either.
Waldmann
we don’t hear much about this in the mainstream or partisan media. you and Bill miht save your country if you can get a wider audience.
i suggest==not criticize– that you get an editor or at least a layman reader to encourage you to write more to fill in the gaps between what you know and what your target audience knows.
too tired myself..tired from trying to explain a much simpler subject to people who don’t want to know. or maybe that’s just an excuse for terminal laziness.