The AMA is Calling for a Relaxing of CMC Opioid Prescription Restrictions
A little history:
In 1980, the Porter and Jick letter to the editor of the New England Journal of Medicine by the Boston Collaborative Drug Surveillance Program stated:
“the risk of addiction was low when opioids such as oxycodone were prescribed for chronic pain.”
It was a brief statement by the doctors conducting the study, taken out of context, and cited many times afterwards as justification for the use of oxycodone.
In a June 1, 2017 letter to the NEJM editor, the authors reported on the broad and undocumented assumptions made as a result of the 1980 Letter on the Risk of Opioid Addiction.. Using bibliometric analysis of the impact of this letter to the editor, the citations of the 1980 letter were reviewed to determine the citation’s portrayal of the letter’s conclusions.
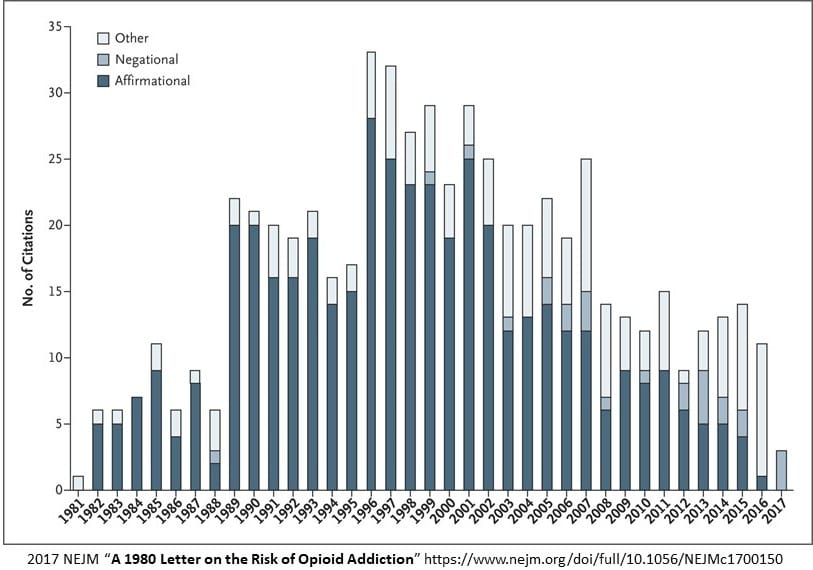
Identified in the bar chart are the number (608) of citations of the 1980 letter over a period of time from 1981 to 2017.
“72.2% (439) of the citations, quoted the letter or used it as evidence addiction was rare in patients when treated with opioids such as oxycodone. 80.8% or 491 of the citations failed to note the patients described in the letter were hospitalized at the time they received the prescription.”
There was a sizable increase of citations after the introduction of OxyContin (extended release oxycodone) in 1995. As the analysis noted “affirmational citations of the letter have become less common in recent years in contrast to the 439 (72.2%) positive and supporting citations of the 1980 correspondence in earlier years. The frequency of citation of this 1980 letter stands out as being unusual when compared to other published and cited letters. Eleven other published, stand-alone, and more recent letters on different topics published by the NEJM were cited at a median statistic of 11 times each.
Citations of the 1980 standalone letter on “addiction being rare” from the use of opioids such as oxycodone failed to mention, the patients administered to were in a hospital setting as noted in the Porter and Jick letter. Overlooked, a mistake, intentional misquote by the people citing this letter?
In 2007 in the pharmaceutical industry, “the manufacturer of OxyContin and three senior executives of Purdue Pharma plead guilty to federal criminal charges that they misled regulators, doctors, and patients about the risk of addiction associated with OxyContin.”
This year, law makers questioned Miami-Luken and H.D. Smith wanting to know why millions of hydrocodone and oxycodone pills were sent (2006 to 2016) to five pharmacies in four tiny West Virginia towns having a total population of about 22,000. Ten million pills were shipped to two small pharmacies in Williamson, West Virginia. The number of deaths increased along with the company and wholesaler profits.
60% of all drug-poisoning deaths in 2013 involved prescription opioids and/or heroin. Among individuals aged 25 to 64 years, deaths from a drug overdose—the majority of which were opioid-related—exceeded motor vehicle collisions as the leading cause of accidental death in 2013. Four in five new heroin users started out misusing prescription painkillers.
The information is out there as to why the abuse of opioids and related drugs is increasing. It is being ignored or argued against as limiting a patients rights to have unhindered access to opioids by doctors and patients alike. Sound familiar, similar to the gun lobby?
Today
AMA Delegates Back Physician Freedom in Opioid Prescribing At best, 20% of all doctors are members and the percentage has been declining. From the meeting; “The CDC’s guidelines on the use of opioids for pain management are well-intentioned, but some insurers and pharmacists have used them to restrict providing and need to be discouraged from doing so, members of the American Medical Association (AMA) House of Delegates said Tuesday.”
And the CDC response as told by one doctor. “a member of a pain management task force being convened by the Department of Health and Human Services. “Draft comments will be coming out in a couple of weeks and will very specifically address the misinterpretation of the CDC guidelines,” he noted. “This is really timely because the comments from the AMA will be extremely important in weighing in [on the issue].”
Doctors do no want interference with decision- making when it comes to patients. At the same time, little has been done to rein in addiction due to prescription opioids which lead to other addictions because prescriptions are expensive or are limited in access. Here is Janet from stopnow blog and who writes about addicted babies due to mothers taking opioids:
More overdose deaths last year than the entire Viet Nam War. The FDA approves sufentanyl 10 times stronger than fentanyl. Yesterday the AMA President was quoted using the same verbiage as Big PhRMA- undertreatment of pain. And now a campaign to undo the CDC guidelines which until they were released doctor education was coming from the drug companies. We need full disclosure – is this funded by Big PhRMA.
Here is a counter argument from a pharmacist where he misapplies the stats to suit his argument:
“it depends what numbers of overdose deaths you are referring to because it is certainly not more deaths due to opioid pain medications. There were 72,000 overdose deaths which includes ALL overdoses from ALL classes of medications. Overdoses from opioids were 49,000 and within that group only 19,354 were from opioid pain relievers. Deaths from fentanyl (illicit) totaled over 29,000, heroin almost 16,000, and cocaine 14,500. (One death could be counted in more than one category, numbers from NIH.) Vietnam war deaths totaled 58,220 versus 19,354 deaths from opioid pain medications. By the way, there were 10,684 deaths due to benzodiazepines, should the CDC mandate doses and days of therapy for those also?
I have no connections with or any payments/gifts from any drug manufacturer. My only concern is that in the national noise of the ‘opioid epidemic’ the focus is on those who abuse opioids and I want to make sure that we still hear the cry of the patient who needs pain relief and who does NOT abuse the medications.”
Yes the pharmacist is correct when he says of the 72,000 deaths only 19,354 can be attributed to opioid pain relievers in 2018. Janet cited the 20 years of Vietnam deaths. The pharmacist conveniently sidesteps the time periods involved here. In three years and if the numbers stay the same (they have been increasing YOY), the numbers of opioid deaths will be slightly less than 20 years of Vietnam if it were to remain at 19,000/year. Four in five new heroin users started out misusing prescription painkillers. Of recently cited 150,000 accidental deaths, 72,000 (a record high) can be attributed to drug overdose deaths, a record high.
And this is ok?
“60% of opioid deaths occur in those who were given a prescription by a physician. The other 40% of deaths are caused by people who obtained opioids by “doctor shopping,” and receive multiple scripts at once. The perceived safety and easy accessibility of these drugs have presented the highest risk for most users, even if they eventually seek out illicit opioids or “street drugs.” In 2014, only 22.1% of non-medical users obtained opioids through a doctor, meaning that the diversion rate of these drugs is very concerning. Many people are getting these medications illegally or without doctor supervision.”
by run75441 (Bill H)
I was in a wheel chair, had a liver transplant, and with a lot of physical therapy and pain I recovered enough to walk and walk away from SS Disability which I could have easily stayed on the rest of my life.
I currently travel extensively but have to take drug tests, have a lot of trouble even getting my Dr’s prescription filled, and while traveling have to drive back home to GA often 1000 miles round trip because my DR already can not prescribe my meds without seeing me face to face.
Most Drs insist on seeing a pain management patient monthly. I have issues which restrict my use of Tylenol and Ibuprofen as well so those are not available. Without these meds I would have no choice but to attempt to re-qualify for disability.
I am already made to feel like a criminal simply for trying to be a productive worker/citizen and function fairly normally with a little help.
Since 2006 when this started I have never once taken more than prescribed, failed a drug test, or failed a pill count which my DR does every time I have an office visit to confirm I have the proper number of pills left for the number of days remaining in that months prescription.
*uck the junkies and abusers but current restrictions are already hard as hell to deal with and maybe a little less so for people who do not travel extensively like I do for WORK!
Garry:
I can not take full strength aspirin or Ibuprofen. It thins the blood too much and my disorder comes back leaving me without platelets. I understand somewhat the issues. Why are you blaming the users and abusers? Lets go back to the letter in NEJM which was abused by doctors citing there was no or little danger of addiction. Why not get angry at Purdue who misled doctors on the danger of addiction from opioids. Is it ok for Miami-Luken to dump millions of tablets in two small communities in West Virginia?
The current opioid addiction crisis is, in many ways, a replay of history. America’s first epidemic of opioid addiction occurred in the second half of the nineteenth century. In the 1840s, the estimated national supply of opium and morphine could have supported a maximum of 0.72 opioid-addicted individuals per 1,000 persons.
Over the next 50 years, opioid consumption soared by 538%. It reached its peak in the mid-1890s, when the supply could have supported a maximum of ∼4.59 opioid-addicted individuals per 1,000 persons. The ceiling rate then began to decline, and by 1920 there were no more than 1.97 opioid-addicted individuals per 1,000 persons in the United States.
The rate today? I beleive is some were in the 5s or near it. It is not coming down any time soon of any magnititude and like I said three years of it are equivalent to 20 years of Vietnam deaths.
Almost the same story as Garry above, but I am retired and no longer try to be a productive citizen. People turn to the streets because their doctors can no longer provide sufficient pain medication to keep them functioning. The guidelines and the way they have implemented them have my doctor afraid to prescribe any painkillers for my husband, because I can only take opiates and two prescriptions for the same household may get his license suspended. My husband can’t always feed himself, because holding a fork or spoon is too painful. But he can take NSAIDS which I can’t. I don’t know if they are trying to scare doctors into not prescribing or what, but my doctor believes that if a drunk driver runs into me and I am killed, because he prescribes opiates for me he will be investigated for overprescribing. Considering that I have been completely pain free for almost 3 hours in the last 15 years, I guess that is overprescribing.
Jane:
Look at how this all came about and the results.
– A letter in 1980-something that said little or no danger. Doctors failed to read the other part of being given in a hospital setting.
– The letter being quoted over 600 times from the time it was written till 2015 claiming opioids will not endanger patients. The citations were lies by doctors and the industry claiming there was little danger.
– Look at Purdue executives who were found criminally guilty of lying about the addictive effects of opioids.
– Look at Miami – Luken who dumped millions of opioid tablets in two little West Virginia towns of ~22,000.
– 58,000 died in Vietnam over 20 years. At 19,000 per year in deaths from prescription opioids, we will surpass Vietnam.
– Look to industry which spent almost $1 billion lobbying state legislatures.
– ~72,000 people died from drug overdoses which is almost 50% of the total accidental deaths in this nation.
It can not stay the same as what it has been as doctors are not taking responsibility for what has been created. The AMA is reacting just like the NRA would if laws were passed restricting bullet-spewing weapons. Here I more industry BS:
“Prior to the introduction of OxyContin in 1995, many physicians were reluctant to prescribe OPRs on a long-term basis for common chronic conditions because of their concerns about addiction, tolerance, and physiological dependence. To overcome what they claimed to be ‘opiophobia,’ physician-spokespersons for opioid manufacturers published papers and gave lectures in which they claimed that the medical community had been confusing addiction with ‘physical dependence.’ They described addiction as rare and completely distinct from so-called ‘physical dependence,’ which was said to be ‘clinically unimportant’ (60, p. 300). They cited studies with serious methodological flaws to highlight the claim that the risk of addiction was less than 1%.” https://www.annualreviews.org/doi/full/10.1146/annurev-publhealth-031914-122957
Lets see what the CMC proposes.
Addiction Rare in Patients Treated with Narcotics January 10, 1980.
To the Editor:
Recently, we examined our current files to determine the incidence of narcotic addiction in 39,946 hospitalized medical patients1 who were monitored consecutively. Although there were 11,882 patients who received at least one narcotic preparation, there were only four cases of reasonably well documented addiction in patients who had no history of addiction. The addiction was considered major in only one instance. The drugs implicated were meperidine in two patients, Percodan in one, and hydromorphone in one. We conclude that despite widespread use of narcotic drugs in hospitals, the development of addiction is rare in medical patients with no history of addiction.
Jane Porter
Hershel Jick, M.D.
Boston Collaborative Drug Surveillance Program Boston University Medical Center, Waltham, MA 02154
Here is the short article which was cited >600 times. The citations claimed addiction was rare. Please note what part of the bolded section was dropped from the citations: “despite widespread use of narcotic drugs in hospitals“
“I want to make sure that we still hear the cry of the patient who needs pain relief and who does NOT abuse the medications.”
As someone who takes them to control the horrific pain associated with chemotherapy-induced neuropathy, this includes me. I’ve been on the same low level of opiods for four years now and have never had a problem.
Fortunately I’m retired, so the time it takes to jump through the extra hoops it takes to get the pain relief I need is not a burden. If I was still working, however, it would be a real impingement on my time. With the drugs, I might add, I would not be functional.
Karl:
The points I bring forth are not about those who need. You, Jane, and Garry are not the issue here. It is the liar-doctors who used a simple letter to profit by it and expand the usage of opioids well beyond what is needed. It is about Purdue, Miami-Luken, H.D, Smith, etc., who have abused their responsibility to the community as a whole in favor of profits. They and the doctors lied to us. Here comes the AMA claiming doctors should be allowed to medicate even when they lied.
Thank you for your comment Karl
The connection in the 1980 statement between the hospital setting and “chronic pain” is simply stunning. It almost seems that they do not know the meaning of the word “chronic.”
I was discussing the use of a new medication with my neurologist and expressed some concern about “dependence.” His reply was that, as a person with Parkinson’s, I am certainly dependent on Levadopa/Carbidopa, right? Dependence is a tricky word.
Run, you are correct as I got defensive and lashed out at the abusers because I have been taking these drugs since 2006 and some days I take less than prescribed and try to fight through the pain with less help.
I understand addiction as I struggled with alcohol earlier in my life and over came that addiction and anyone who is addicted the first step in to admit it and take responsibility.
My point is the laws are already so restrictive that if they tighten the laws any more than they are people like me who don’t abuse the drugs but truly need them to make a productive life will have no alternative but to either live in pain or stop trying and go back on disability. I have to drive from Miami to Georgia and turn around and drive back in excess of 1,000 miles driving because my DR is required by law to see me face to face even though he has been my Dr for years and years.
I don’t know what the answer is but every time I read an article like this I think here is another person who truly would like to make the use of these drugs illegal.
Run, I was the type person before ending up in a wheel chair who would not take an aspirin or any medicine period and laughed at people who said they needed this or that pill. I ate a lot of words when learning how to WALK again.
The darn laws are super restrictive right now and my Dr’s hands are virtually tied on this type prescription.
Garry:
I do not know if they will make them tighter. If you read the 2017 study on the numbers of citations used by doctors in 1980, hundreds of doctors flat out lied and construed what Jinck and Porter said in their letter to the NEJM. Purdue and other manufacturers campaigned on the difference between addiction and physical dependence.
“opiophobia,” physician-spokespersons for opioid manufacturers published papers and gave lectures in which they claimed that the medical community had been confusing addiction with ‘physical dependence.’ They described addiction as rare and completely distinct from so-called ‘physical dependence,’ which was said to be ‘clinically unimportant’ They cited studies with serious methodological flaws to highlight the claim that the risk of addiction was less than 1%.”
I understand the issues; but going back the other way and giving doctors the freedom to do as they please, has not worked and they refuse to take responsibility for being one of the causes of this epidemic. .
Run,
Karl, Gerry and I are not the issue, but we have been harmed by every action taken to date.
I haven’t seen anything at any time that leads me to believe that any of the people deciding on what actions to take even know that people like us exist. They only see addiction, which they conflate with physical dependence, and decide that cutting off the supply will fix the problem. If they do anything else it has not been effective at fixing the problems of overdose and addiction.
I stopped believing they wanted to reduce the number of addicts and overdoses when they came out with the same failed “solutions” for the third time.
Jane:
I know you, Garry, and Karl are not the issue; but it has gotten so bad, they just can not prescribe Opioids the same as Metoprolol, Lisinopril, Prilosec, etc. The doctors have not taken up the responsibility and the corporation are feeding off of the profits made. Purdue flat out lied on the impact of Oxycodone in 1995. Doctors who used that 1980 letter and did not mention opioids were used in a hospital setting flat out lied to. Here are the facts and mostly why we have an epidemic on our hands.
“60% of opioid deaths occur in those who were given a prescription by a physician. The other 40% of deaths are caused by people who obtained opioids by ‘doctor shopping,’ and receive multiple scripts at once. The perceived safety and easy accessibility of these drugs have presented the highest risk for most users, even if they eventually seek out illicit opioids or ‘street drugs.’”