Free Medicine Distribution Impact on Health Care Costs
This is an abbreviated version of a Canadian trial which examines whether eliminating out-of-pocket costs would improve the health of people taking the medications by making drugs less costly. The greater impact was amongst lower income participants who may not take drugs as prescribed to lengthen a refill timetable. The elimination of out-of-pocket medication costs resulted in lower and reduced total health spending by a median of $1641 and a mean of $4465 over 3 years. This suggests the elimination of out-of-pocket medication costs for patients could reduce overall costs of health care.
For more detail, please read the full report. Not terribly long and an easy read.
JAMA Health Forum – Health Policy, Health Care Reform, Health Affairs, JAMA Network, Nav Persaud, Michael Bedard, and Andrew Boozary.
Objective: The quintuple aim is to reduce costs, improve outcomes, improve patients’ and clinicians’ experiences, and promote health equity.
Health inequities associated with avoidable disparities in outcomes based on income, racism, and other forms of discrimination are estimated to contribute substantially to health spending through poor outcomes for disadvantaged individuals. These inequities can be reduced with better access to basic necessities and health care, including preventive care. Fortunately, you can now access a drug resource list online to make it easier for you to order the prescription drugs that you need.
It is thought the elimination of out-of-pocket medication fees on total health care costs addressing cost-related nonadherence has the potential to do so. AB: This would seem logical to me.
Not taking medicines as instructed due to cost, is more prevalent among people with low incomes and is associated with poor health outcomes. Broader prescription drug insurance reduces use of other health care services and has a positive impact on patient outcomes. Coverage gaps or caps on drug insurance generally led to worse outcomes.
The CLEAN Meds (Carefully Selected and Easily Accessible at No Charge Medications) trial examined the effects of free distribution of essential medicines among people experiencing cost-related nonadherence in Ontario, Canada. Physician and hospital care services are universally funded by public payers but do not include prescription medications.
In this (secondary) analysis of the CLEAN Meds trial, a 36-month trial reports the results of free medicine distribution on health care costs and health care encounters among primary care patients experiencing cost-related nonadherence.

Included were adult (≥18 years old) primary care patients who reported cost-related nonadherence (not filling a prescription or not taking as instructed to make a prescription last longer due to the cost) in the 12 months prior to study participation between June 1, 2016, and April 28, 2017. Primary care clinicians identified potentially eligible patients.
A total of 1130 patients were assessed for eligibility, and 786 (mean [SD] age, 51 [14] years; 421 [56.4%] female) were randomly allocated between June 1, 2016, and April 28, 2017. Of those randomized, 39 patients (5.0%) did not consent to the use of health care administrative data, including 13 of 395 patients (3.3%) in the free distribution group and 26 of 391 patients (6.6%) in the usual access group; the characteristics of those included were similar to those in randomized controlled trials. This analysis compared 382 patients in the free distribution group and 365 patients in the usual access group. There were 8 deaths (2.1%) in the free medicine distribution group and 14 deaths (3.8%) in the usual access group (P = .16).
Eliminating out-of-pocket medication fees was associated with a lower median total health care spending over 3 years of $1641 (95% CI, $454-$2792; P = .006.
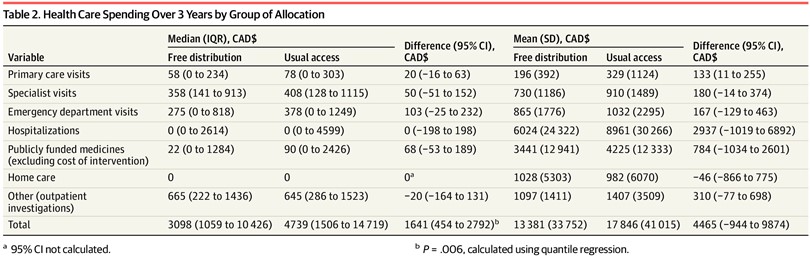
Free distribution was associated with a lower number of participants with very high total health care costs (see Jama Health Form above). Hospitalizations represented the largest cost in both groups (Table 2). Between the free distribution and usual access groups, there was not a statistically significant difference in the number of hospitalizations (mean [SD], 0.9 [1.6] vs 1.2 [3.0]; P = .08) or the rate of being hospitalized at least once (38.7% vs 44.1%; P = .14) (Table 3).

There was no statistically significant reduction in primary care visits, specialist visits, and emergency department visits (Table 3). A relatively small number of participants (10 [2.6%] with free distribution and 17 [4.6%] with usual access) had total health care costs greater than $60 000 (see Jama Health Form above). Mean total costs were $4465 (95% CI, −$944 to $9874) lower over 3 years, or $1488 (95% CI, −$315 to $3291) lower per year.
The findings suggest the promoting of health equity by improving medicine access can reduce overall health care costs. Adding to prior studies showing the free medicine distribution improves the experiences of patients and clinicians. Free medicine distribution may help achieve the quintuple aim that includes both reducing health care spending and improving health equity or fairness in health care and outcomes by ensuring that financial means are not a barrier to realizing the benefits of medicines.
https://fred.stlouisfed.org/graph/?g=17yyj
January 15, 2018
Life Expectancy at Birth for United States, Canada, Mexico and Brazil, 2017-2021
https://fred.stlouisfed.org/graph/?g=17yyw
January 30, 2018
Infant Mortality Rate for United States, Canada, Mexico and Brazil, 2017-2021
The findings suggest the promoting of health equity by improving medicine access can reduce overall health care costs. Adding to prior studies showing the free medicine distribution improves the experiences of patients and clinicians….
[ Excellent. ]
my comment was deleted,probably by a misplaced keystroke opening up an ad. decent site design would not let this happen.
basic point was that conflating social security with medicare costs is a standard lie of the enemies of Social Security.
please delete my comment above. the lost comment appeared on the thread where it belongs.. part of it anyway.
I see this cost impact almost every trip to the pharmacy. I have always had good medical insurance, with drug co-pays between zero and $10 for a month’s supply, most of the time it was a 100 day supply. Even when I was taking a lot of medication, I could afford it. And almost every time I went to pick up a refill there was someone there who had just been told their medication costs were in triple digits.
30-40 years ago even a $100 co-pay was unaffordable, now it is in the $3-600 range. Even when I don’t hear the price they are quoted and see the shock on their face, I see people trying to evaluate which medication they can do without. One time it was a mother whose medications were for a toddler, and the pharmacist was talking to the doctor to see if there was a cheaper drug to use. Another time they were trying to evaluate the medical effects of delaying starting one drug for another week, or using a half tablet. These are working people with employer health insurance for the most part. Smaller business with a lower cost policy giving lower benefits than I always had. You are not supposed to hear what they are saying, but you can’t help it. And you can’t help them either.
Jane
well, maybe we could. we know how to cut costs. bur the same criminals who control Congress won’t let us do it. Unless we make them. WE still have a democracy and we can still vote Congress persons out of office. But it would take serious work and organization…and talking to people we might not otherwise like or agree with.
Now the chances of you or me doing this are almost zero. But if a few people got together and said “this isn’t working” and found a way to talk to people in other parts of the country who have gotten together ans said “this is not working,” there is a fair chance we could eventually get smart enough and strong enough…
but we might have to first learn how to get along with each other.