A Randomized Clinical Trial, Clinical Pharmacy, and Pharmacology
Will a high dose of Ivermectin for 6 Days impact Covid?
As a biochemist, I find the argument of a lack of mechanism for Ivermectin as a justification for prescribing it for COVID particularly pernicious. While it is correct to say that we didn’t know the mechanism for aspirin for decades after we knew it worked (one could say the same about the smoking and lung cancer), that’s not a logical basis for prescribing a drug.
The gold standard is a double-blind, randomized, placebo-controlled trial. Such was reported, February 20, 2023.
“Effect of Higher-Dose Ivermectin for 6 Days vs Placebo on Time to Sustained Recovery in Outpatients With COVID-19: A Randomized Clinical Trial, Clinical Pharmacy, and Pharmacology.”
JAMA | JAMA Network, Susanna Naggie, MD, MHS1,2; David R. Boulware, MD, MPH3; Christopher J. Lindsell, PhD4.
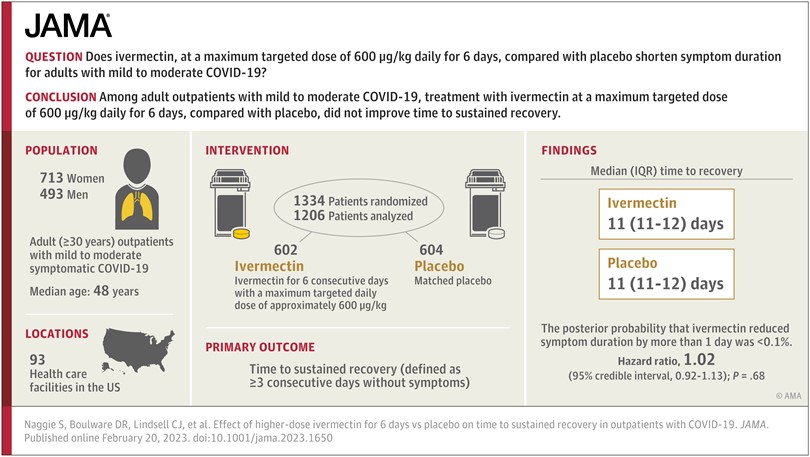
Question: Does ivermectin, with a maximum targeted dose of 600 μg/kg daily for 6 days, compared with placebo, shorten symptom duration among adult (≥30 years) outpatients with symptomatic mild to moderate COVID-19?
Findings: In this double-blind, randomized, placebo-controlled platform trial including 1206 US adults with COVID-19 during February 2022 to July 2022, the median time to sustained recovery was 11 days in the ivermectin group and 11 days in the placebo group. In this largely vaccinated (84%) population, the posterior probability that ivermectin reduced symptom duration by more than 1 day was less than 0.1%.
Meaning: These findings do not support the use of ivermectin among outpatients with COVID-19.
Sounds about right to me. But it might be important that the experiment was conducted on “this largely vaccinated (84%) population,” reduces its usefulness. If I have two drugs which are equally effective, I might not get a result that shows adding one or the other drug to the treatment increases the effectiveness of either, but that does not rule out the possibility that either drug, taken alone, is an effective treatment.
For what it is worth, I do not believe Ivermectin is useful in treating or preventing Covid, but this study does not seem to establish that it is not.
[for what it’s worth, I do not take aspirin either. no doubt it “works” but in my experience, so far, so does ignoring the pain.]
A biochemist. LOL. Shouldn’t be dabling in medicine. You’re not qualified.
He is not dabbling in Medicine. He is dabbling in how a med comes to market and is approved for use by humans. I will repeat what was said in the post. I want to make sure you understand what was said. Not even a doctor can say it works until a trial is performed.
“The gold standard is a double-blind, randomized, placebo-controlled trial. Such was reported, February 20, 2023.”
Effect of Higher-Dose Ivermectin for 6 Days vs Placebo on Time to Sustained Recovery in Outpatients With COVID-19
A Randomized Double-Blind Clinical Trial
It’s called sherry picking from someone unqualified in medicine. Simple.
If you need real studies http://www.ivmmeta.com
But if you’re not an MD you shouldn;t even try reading those.
@loaner,
The reference cited in the post is a refereed journal. Your link is not refereed. That’s called cherry-picking. As a scientist and medical school professor, I know the difference.
loaner:
If you can not write properly in English, you should not be challenging anyone. Spelling and punctuation are important attributes for someone to have, portraying themselves as an authority, and then offers up unrefereed documentation. You have no foundation for your opinion or documentation.
LOL! Ten of the co-authors are not MDs. Furthermore, this isn’t “dabbling in medicine,” this is a clinical trial.
Just a reminder. This post isn’t about me. Anyone who makes it about me and/or engages in personal attacks will have their post deleted.
At severe risk to my continued life on AB: whatever the merits of the controlled study, all it shows is that Ivermectin does not “reduce time to sustained recovery when used to treat previously vaccinated patients”. It does NOT say anything about it’s value as a stand-alone treatment, or treatment of unvaccinated patients.
I could be wrong about this ..i don’t know the details of the study and i am not a doctor or even a scientist. But all the arguments i have heard so far are arguments “from authority” which the author of the present post has described as “deserving contempt.”
a “gold standard” double blind study doesn’t mean a damn thing if it does not measure what you think it does.
I am troubled that the medicine was only used for six days while time to recovery was eleven days for both treatment and control groups.
could easily be an explanation for that, but i haven’t heard it.
life being short and all, we all accept “authority” in considering an argument, but if we have doubts, we turn to the argument itself and see if, to the best of our understanding, it holds up. It helps if we actually know what the argument is about.
Coberly:
You have “no” basis other than an opinion for your commentary. Covid rapidly multiples and moves through the body quickly. One does not have weeks to block Covid from infecting the lungs and the rest of the body. It is a matter of days.
I know we have to hold your hand and ask first if you understand before we post factual evidence, which the result of the evidence coming from medical trials and refereed documentation. That the “witch doctors” to which you have some type of allegiance to, keep insisting there is value to using Ivermectin is not evidence.
Their commentary foundation is supposition, conjecture, and innuendo to which you should not be ascribing too.
A Rampage Through the Body April 2020
Psst: I deleted your last comment. It was not needed as everyone knows what you believe.
Angry Bear does not extinguish life, we can remove the ability of the person to comment if needed.
For those who are seriously interested in meta-analysis of ivermectin and COVID-19, you should read and understand this and associated links (references 1-4):
ACochrane meta-analysis of 11 eligible trials examining the efficacy of ivermectin for the treatment of COVID-19 published through April 2022 concluded that ivermectin has no beneficial effect for people with COVID-19.1 Since May 2022, an additional 3 large randomized clinical trials including several thousand participants have been published, each reaching a similar conclusion. At a Higher Dose and Longer Duration, Ivermectin Still Not Effective Against COVID-19
Somewhere lost in my saved Twitter info about COVID was a rough analysis of the various plausible early studies about Ivermectin and COVID. The author, after eliminating obvious forged data, and studies that had questionable or unclear methods (hey, let’s eliminate fatalities from the Ivermectin group but not the control group), still came up with about a 50/50 split on studies that showed a positive effect (however minimal) and ones showing no effect whatsoever.
Then he noticed something: the negative studies all came from the US and Europe, while the positive studies came from countries like India and Brazil, locations where the parasitic worms that are normally treated with Ivermectin are endemic. Their working theory was that, during the height of COVID, treating an undiagnosed parasitic infection would increase survival rates among COVID patients.
Unfortunately, “undiagnosed” is the key word, because none of the positive studies looked at co-morbidities and/or other afflictions of the treated, including the parasitic worms normally treated by Ivermectin. TLCR; Ivermectin is good for treating parasitic infections, and if you happen to have one while suffering from COVID, improves your survival chances by treating the parasites, not COVID, allowing your body to better fight off the viral infection.
@FG,
Interesting and provocative speculation! Seems plausible to me. Wouldn’t be surprised if there’s a study underway somewhere to address this.
There are certainly a number of co-morbidities that affect the outcome of COVID-19. One is hypertension. It appears that being treated for hypertension isn’t a co-morbidity. By extension, then, having a parasitic worm infection might be a co-morbidity while being treated for an infection wouldn’t.
@FG,
I found some papers in refereed journals and one on bioRxiv, and the claims (which have a high speculation-to-data ratio) are contradictory. Some claim that parasite infection could be protective for COVID-19 by suppressing cytokine storms. Others claim that parasite infections blunt the immune response, increasing the severity of infection and reducing vaccine response.
I shared your post with the director of our vaccine center, where I was enrolled in the Moderna phase III trial. He’s an expert on COVID and on parasitic infections. Here’s his response:
“I do not consider Twitter to be a robust peer-reviewed platform. Certainly, if you have multiple infections they may have additive negative health effects, but I have not seen any data in the peer-reviewed platforms that demonstrate this specifically for co-infections of parasitic helminths and SARS-CoV-2. Appropriate to state that persons with documented parasitic helminth infections should be treated.”
I’m not disagreeing; I saw the thread in early 2022, and at the time no studies re:Ivermectin/COVID were looking at the parasite infection angle, or even checking medical histories/followups to determine if such was the case. I get the feeling that such co-infections were rare in quality studies like the one cited here, and not looked for in the more credulous papers that were bruited about at the time.
Sounds like the good doctor is afflicted with the same syndrome that has plagued Medicine since the days of Dr Semmelweiss.
Reader FG identfues a possible reason some studies showed a positive effect of Ivermectin was that some patients were infected with worms as well as Covid.
The good Dr does not deny the possibility but needs to pooh pooh the source.
Dr Ignaz Semmelweis, a Hungarian physician newly appointed as an obstetrician at a hospital in Vienna, wants to know why so many more women are dying there under the care of doctors than when attended to by midwives. His controversial discovery, which led to his expulsion from the medical establishment and a mental breakdown, is the subject of Dr Semmelweis, a new play opening in London in late June, starring Mark Rylance.
coberly:
I already wrote on Maternity and it was used by one organization which asked me to write on the topic. Late to the game. FG comment had a positive comment(s) which was not negative, but an explanation of why maternity occurrence was dangerous for women.
Just to be clear, this is not a discussion.
Bill
I really have no idea what you are trying to say, but since you appear to have no idea what I am trying to say, let’s just call the whole thing off.
Fraud Guy:
I broke this into paragraphs for easier reading. Otherwise, this makes sense to me. As you know and as I believe, Covid is a virus. I do not know of meds which will kill a virus and is given meds, you are being treated for other symptoms resulting from the virus.
Joel is the resident expert. I concede to his analysis.
@Bill,
“I do not know of meds which will kill a virus”
Nor do I. The closest I can think of to something like that is acyclovir, which is used to treat herpesviruses and, I believe, is the most widely prescribed and clinically effective antiviral on the market. It doesn’t actually “kill” the virus so much as kill virally infected cells.
Joel:
Kill the host and the parasite, virus dies or is flushed out of the system(?). That makes sense.
@Bill,
Yes. The key is that acyclovir is a kind of “prodrug,” and can only be activated by an enzyme expressed by the virus. The activated drug acts as a poison for DNA replication only in infected cells.
Joel:
Is the Covid vaccine joining with the Covid RNA thereby blocking from doing so with cells?
Joel:
Thank you for detailing this in a better and technical fashion to which we can better understand.