The Future of Medicare and Advantage Plans
This post comes by way of Joel Eissenberg’s Facebook blog and is an edited recital of Juan Cole’s presentation at Informed Comment. “Stop Wall Street from Grabbing Traditional Medicare,” F. Douglas Stephenson
__________
I am going to add to Joel’s depiction of the future as I too had heard of the coming attempt to force seniors into the commercial healthcare program – Medicare Advantage. This is the only time I will tie the words Medicare and Advantage together. I have written several times on Medicare and the Advantage pickpocketing of healthcare for seniors by commercial healthcare. Commercial healthcare in this form is certainly an advantage, an advantage to commercial healthcare doctors, hospitals, and clinics; commercial healthcare insurance; and Wall Street investors.
Some History
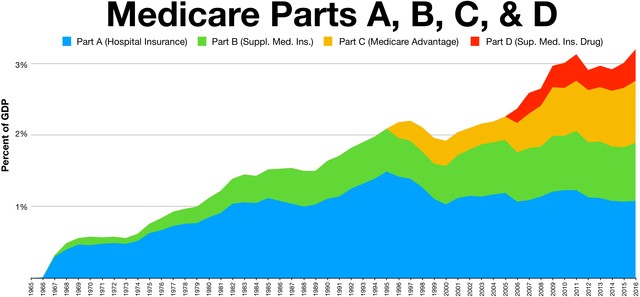
The diminishing numbers of Baby Boomers are “still” a gold mine waiting to be mined by Wall Street and the healthcare industry. The only thing standing in the way of more profits is Medicare setting the prices to be paid to hospitals, clinics, and doctors. How rich is this vein of gold? Medicare programs represent >3% of GDP as depicted in the graph below.
When you go to the doctor’s office and discover healthcare issues during the visit, they code the issues to identify them and commercial healthcare insurance pays the doctor according to the codes. The more codes a doctor can assign to a patient the higher the compensation is in both commercial healthcare plans, Advantage, and Medicare. Typically, a payment by commercial healthcare is 175 to 300% of Medicare payments. Advantage plans are less costly. Less costly only because Congress has made it this way in a giveaway to Advantage insurance companies.
Advantage has been known to code patients higher than what is necessary and if not treated the following year, will still charge CMS. A patient has to be aware of how they are coded and why. Most seniors are not aware of what service they are paying for in a visit. The current battle between Advantage and CMS is the alleged over charging of healthcare by Advantage companies to the tune of $billions. CMS has documented the issue and is “still” attempting to collect.
Advantage plans also cherry pick their patients, the less costly patients. If you are costly, you may find your fees increasing.
An Example of Coding
I have been coded having high cholesterol. Yet while having open heart surgery, my cholesterol was 104. Most recently it was 123. When I challenged the coding, the cardiologist admitted I was technically correct about not having a cholesterol problem. I do have an issue with triglycerides. Yet every time I am in the office the NPs ask about my cholesterol.
From an expert on healthcare for seniors, Nancy Altman;
“Medicare Advantage is a hustle designed to allow for-profit corporations to suck up public dollars.”
How Big is the Healthcare Market for Seniors?
The breakdown in the graph details shows the percentage of seniors in each segment of Medicare and Advantage programs as related to GDP. Note the growing percentage of Advantage plans which are known to be more convenient for seniors. A one stop shop for seniors.
Except as experienced by many seniors, once you go with Advantage plans, you may not be able to acquire a Medicare Supplemental plan if you return to Medicare. Typically, Advantage plans are tied to one healthcare organization which may be geographically limited. If you go elsewhere, you may experience higher prices. Medicare, Supplemental, and Part D can be used anywhere in the US.
Until you get older, Advantage plans “can be” less costly than Medicare.
Joel Details the Future
For now, you can choose traditional Medicare or Medicare Advantage. If you plan to remain where you are and like the healthcare in your network, Medicare Advantage may be better for you. But if you need flexibility, traditional Medicare offers more choices.
It looks like the financial investment business has its sights set on eliminating traditional Medicare by 2030 and forcing everyone onto insurance that is as bad or worse than Medicare Advantage:
“The Center for Medicare and Medicaid Services “Innovation Center” recently announced that by 2030, they will move all traditional Medicare enrollees into a “care relationship” with a 3rd party private, for profit middleman, labeled a “Direct Contracting Entity (DCE) without seniors’ knowledge or consent, and without Congressional oversight.
Every enrollee in traditional Medicare should take note of the dangers. A program titled the Global and Professional Direct Contracting model in a little-known government agency known as the Center for Medicare and Medicaid Innovation (“The Innovation Center”) is already moving them, without their knowledge or consent, to “risk-bearing,” for-profit middlemen known as Direct Contracting Entities (DCEs). The goal: to end what’s left of traditional Medicare as a public, non-profit social/health insurance program.
Simply put, it proposes that a “risk-bearing,” for-profit middleman manage health care for traditional Medicare beneficiaries, just like Medicare Advantage plans are for seniors who have signed up for Medicare Advantage plans. The difference is that while 26 million seniors have voluntarily signed up for a middleman when they chose Medicare Advantage, the 38 million seniors in traditional Medicare have not.
How do you get seniors who have specifically chosen traditional Medicare to switch to a non-traditional Medicare-Advantage-like plan with a mysterious name like “Direct Contracting Entity”?
You don’t tell them!
You lure their primary care providers to participate in a DCE by promising the doctors much better Medicare reimbursement rates and more time with their patients, and once the doctors sign up with a DCE, all their patients are automatically “aligned” by CMS with the DCE the doctor has chosen.
The DCE sends patients a letter they are likely not going to read or understand, and presto! Millions of seniors previously on traditional Medicare now belong to a DCE. That’s how DCEs leverage and monetize the doctor-patient relationship for the profit of private corporations, oligarchs and other Wall Street entities.”
Thanks, Joel, run
This should be front page
Ken:
Been writing on Advantage programs most of this year using Kip Sullivans research in a paper supporting issues with Advantage and healthcare payments. Not sure it is read much here or elsewhere. I started writing on healthcare with Maggie Mahar when she was here. I did her editing too.
Everything in the beginning of this post, I have written on here at AB in numerous posts. The graph and the future predications are Joels and are excellent in prediction.
Thank you for commenting.
The first political move in all this I call ‘leg breaking.’ First Congress has to prohibit the government from providing a service or product. I call this ‘leg breaking’ in honor of a cat I once owned called ‘Boogie.’ Boogie was a famous mouser in cathood lore. The first thing Boogie did to his victim was break one of it’s rear legs. Thus crippled Boogie played with his victim for a while then, when bored, killed it by crushing its skull. He’d leave the dead mouse on my doorstep. A form of homage I suppose. Anyway, leg breaking is the first goal to accomplish when one if attempting to privatize a public asset or purpose. Capitalists have grown immensely more powerful by first ‘breaking legs’ of government. Ronald Reagan was a blue ribbon, first class ‘leg breaker’.
Sorry.
I have had Kaiser Medicare Advantage for 7+ years and I am very happy with it.
I won’t even consider anything else.
Kaiser provided excellent treatment for colon cancer (surgery, chemo) and the total cost to me was $2500.
Dave:
Was waiting for your comment.
I paid for your care also in the amounts of money Advantage has swindled. Commercial Advantage healthcare is more thievery. To wit, 6 infusions = ~$200,000 commercial prices to which Medicare paid ~26%. I paid for two lunches at $10 at the cancer center. Not dying either if someone mistakes what I wrote here.
@dave,
Good on you.
Sorry, not everyone can get Kaiser MA. Sorry, not everyone can work with the narrow provider networks enforced by MA.
They are not so much signing up doctors as they are signing up medical provider corporations. That is, part of the move that has been going on for a few decades and accelerated over the past 20 years to 10 years is making doctors employees. It’s has been done as the administrative work has grown well beyond what a single practitioner can manage. The act of digitizing all records has also aided in this transition. The act of connecting all providers via the net has made “group practice” seem the logical choice.
Of course with all this movement what is being lost is the actual job of applying the knowledge of health and healing to the person in need of that knowledge.
I theorized ages ago that computers would ultimately dictate how one thinks. Dictate the flow of thought and thus action. This is because the flow of the software dictates how one interacts with it which will dictate how one interacts with the events that are required in order to fulfill the dictates of the software. The software only asks questions, and does so in an inflexible manor.
The doc are simple employees on an assembly line. Not much different than any other job. The doc’s don’t see it. That is what has been so clever about all this. That the doc’s still think they are in charge.
@Becker,
“The doc are simple employees on an assembly line. Not much different than any other job. The doc’s don’t see it. That is what has been so clever about all this. That the doc’s still think they are in charge.”
There’s a lot of truth to that. I’ve been teaching medical students (future docs) for 35 years. A few years in, I referred to medical school as a “trade school” in front of a bunch of white coats. I was told that the acceptable term is “professional school.” Whatever used to pass for scholarship in training med students at our medical school is rapidly being drained out of the curriculum, as the focus is passing Step 1 and getting into the clinic.
Watson is already better at reading images than radiologists. A lot of tasks that used to be done by physicians are being done by physician’s assistants and nurses. Look for that to continue, as the downward pressures on insurance payouts increase. Some docs see it, but many don’t.
Daniel:
“‘group practice’ seem the logical choice.”
It is almost the only choice as the ACOs are buying up clinics and group practices. ACOs have become strong enough to reject insurance companies and or drive pricing in certain areas of the country. If you have a certain policy other than the preferred policy, a patient may pay more.
With Medicare, the prices remain the same to my knowledge.
The coding is pigeon holing. Get the wrong code and the claim could be rejected. One doctor I had temporarily jumped the process and prescribed a procedure out of the normal order. I showed up and they did the procedure and insurance refused to pay it. They put it on my bill and I asked U of M to remove it as I have no authority on these matters and follow the advice of the doctors. About $15,000 “list” they owned.
you are lucky, i had a very minor procedure early this year, prior to insurance, it was about $80,000, after all the insurance coverage, i ended up pay $7500 for that minor procedure. oh and the doctor worked for the hospital where the procedure was done. his part of that bill? less than $1000
[After the New Deal revisionism explained at the link, then the rest was inevitable – slippery slope and all that.]
https://www.nytimes.com/1986/07/04/us/blue-cross-tax-status-is-challenged.html
BLUE CROSS TAX STATUS IS CHALLENGED
Special to the New York Times
“…
The differences between Blue Cross-Blue Shield health insurance plans and commercial health insurers may not be great enough to justify Blue Cross-Blue Shield’s tax-exempt status, the General Accounting Office has concluded.
In a draft of a report to be released next week, the office, an investigative arm of Congress, said similarities between Blue Cross-Blue Shield and commercial health insurers diminished the justification for the tax-exempt status.
The report said agency officials agreed with the Internal Revenue Service ”that the Congress needs to decide whether the current exemptions are warranted.” $340 Million Tax Saving Congressional estimates put the tax saving for Blue Cross-Blue Shield at about $340 million a year.
A tax bill passed by the House would revoke that tax-exempt status; the Senate version of the bill would retain it…”
*
[We know how that went. The original back story has been forgotten. Blue Cross administrative workers went to Vegas for their conference which later showed up on 60 Minutes. I also do not recall whether it was revealed on 60 Minutes that Vegas was the lowest cost venue for large conferences in the US at that time. I attended the CMG (Computer Measurement Group) International Conference in Vegas during December 1986, but we were not allowed to host another event there until the current century because computer performance analysts do not waste much money on gambling. In any case, then it only took a few more years for BC/BS companies without their tax exemption to be allowed by the BC/BS Association to go for profit. It then naturally followed that they go public and consolidate, all in the name of market efficiency.
Just because we broke it, then that in no way implies that we know how to fix it. Actually, quite to the contrary.]
Required reading for those that think the commercials are the worst thing about Medicare Advantage. Particularly the ones with the most overrated player in the history of football, Joe Namath.