The Importance of Rural Hospitals
I did present data on rural hospitals in the past in rewrites. It has been a while since I wrote much on healthcare as it takes a lot of investigation to do so. With Dan around and other writers, I was able to do the research on the topic. I am not complaining as I am happy to see many of your comments. Joel has also provided help and excellent presentation writing and in comments. The problem of providing healthcare, healthcare in rural cities, and healthcare in inner cities still exits. It costs and the funding is not adequate.
Problems and Solutions for Rural Hospitals – Saving Rural Hospitals
The Importance of Rural Hospitals (2024 Data)
There are two very different types of hospitals in the U.S:
(1) small rural hospitals, and
(2) urban and large rural hospitals.
There are over 1,000 small rural hospitals, representing nearly one-fourth of all the short-term general hospitals in the country, but they receive less than 3% of total national spending on hospitals.
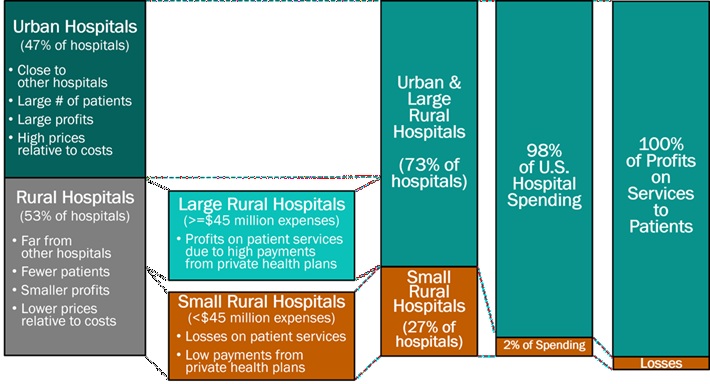
Small rural hospitals provide most or all of the healthcare services in the small communities they serve. Not only do they provide traditional hospital services such as emergency care, inpatient care, and laboratory testing, many of them also deliver primary care and inpatient rehabilitation services. Also, a majority of the communities they serve are at least a half-hour drive from the nearest alternative hospital. Many communities have no alternate sources of health care.
The services provided by small rural hospitals are also important for residents of urban areas. Most of the nation’s food supply and energy production comes from rural communities. Farms, ranches, mines, drilling sites, wind farms, and solar energy facilities can not function without adequate and an available healthy workforce. People are less likely to live or work in rural communities not having an emergency department and other healthcare services. Many popular recreation, historical, and tourist sites are located in rural areas. Visitors to those sites need access to emergency services if they have an accident or medical emergency.
The Crisis Facing Rural Healthcare
Small rural hospitals are struggling to survive and rural communities suffer harme. A majority of small rural hospitals are losing money delivering patient services. the result being 100 rural hospitals closing in the past decade. Most of these were small rural hospitals. In most cases, the closure resulted in the loss of both the emergency department and other outpatient services. Residents of these communities travel much farther when they have an emergency or need other healthcare services. This increases the risk of death or disability when accidents or serious medical conditions occur. The risk of health problems increases, goes undiagnosed or inadequately treated due to lack of access to care.
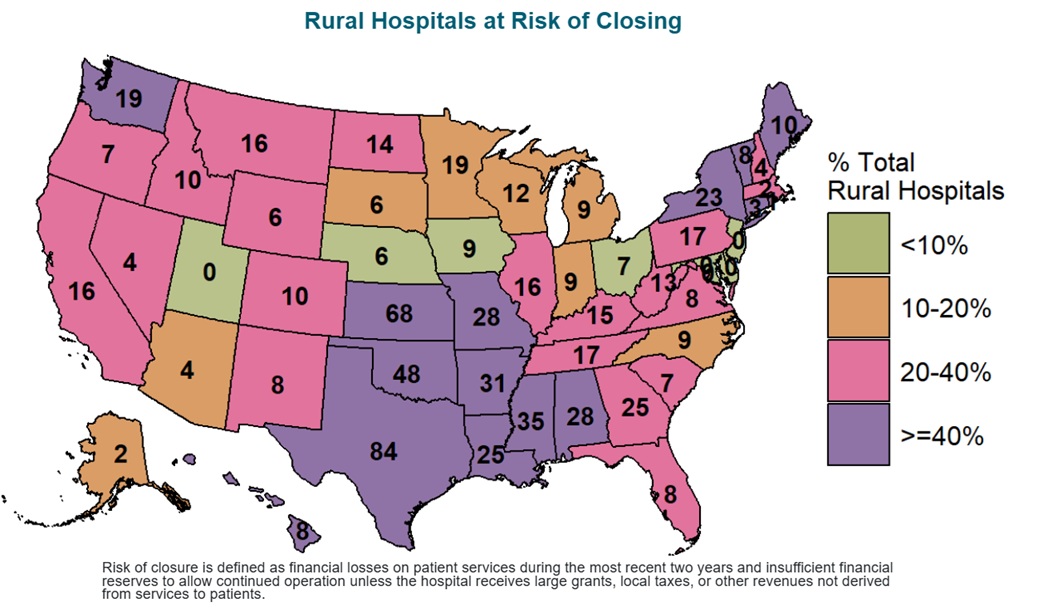
Over 700 rural hospitals (one-third of all rural hospitals in the country) are at risk of closing in the near future. Over 300 of these hospitals are at immediate risk of closing. A majority of the at-risk hospitals are small rural hospitals located in isolated communities. The loss of the hospital will severely limit access to health care services. Reoccurring closures places millions of people at risk and directly in harm’s way if these hospitals close. In all parts of the country people could be affected through the impact on workers in agriculture and other industries.
The Causes of the Financial Problems at Small Rural Hospitals
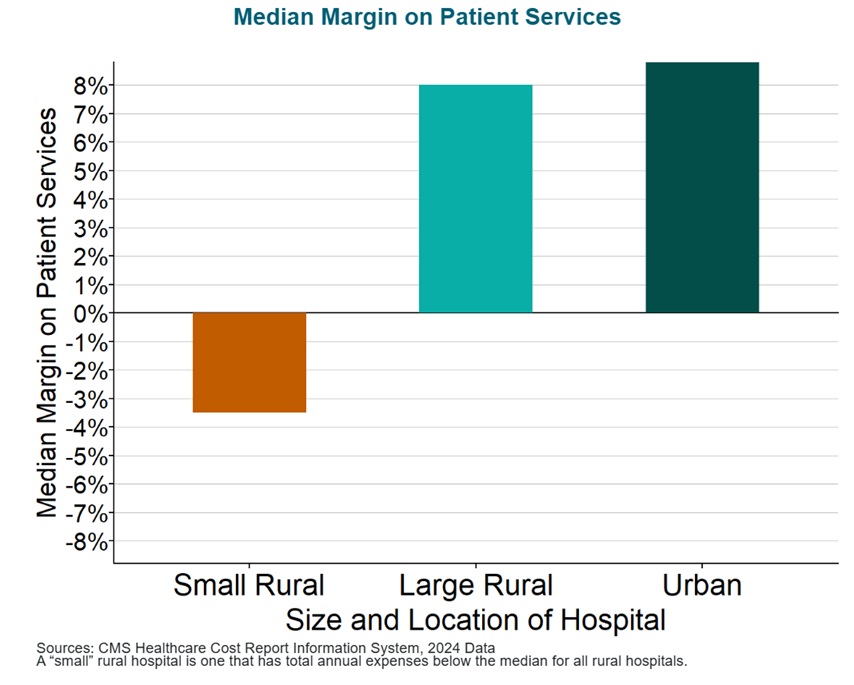
Small rural hospitals are being forced to close because they are not paid enough to cover the cost of delivering care to patients in rural areas. Most small rural hospitals lose money delivering services to patients. Most urban hospitals and larger rural hospitals make profits on patient services. The traffic does not cover the costs. In which case, governmental subsidies would help sustain them.
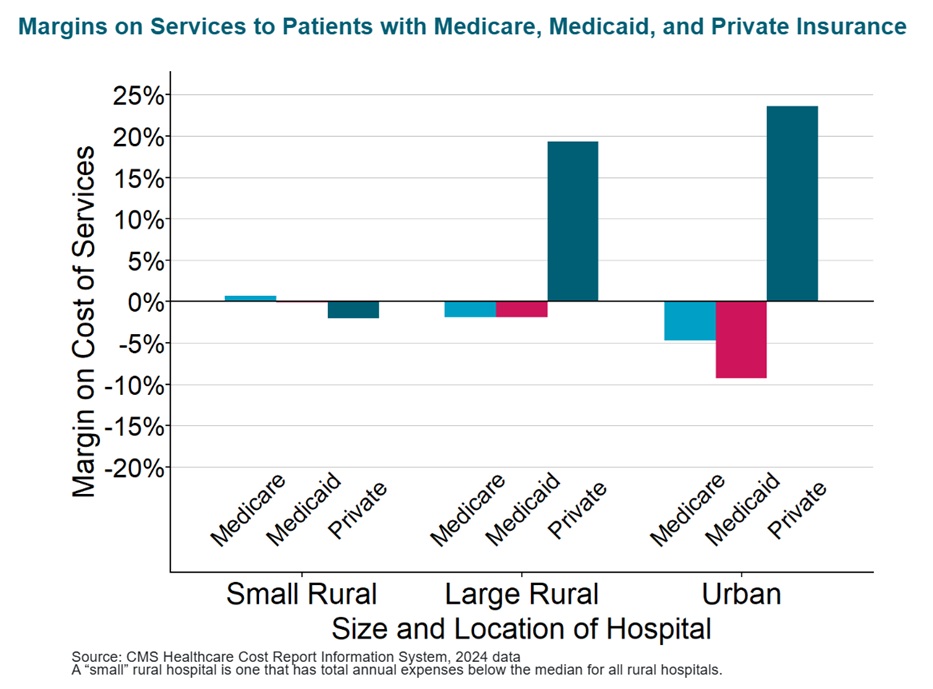
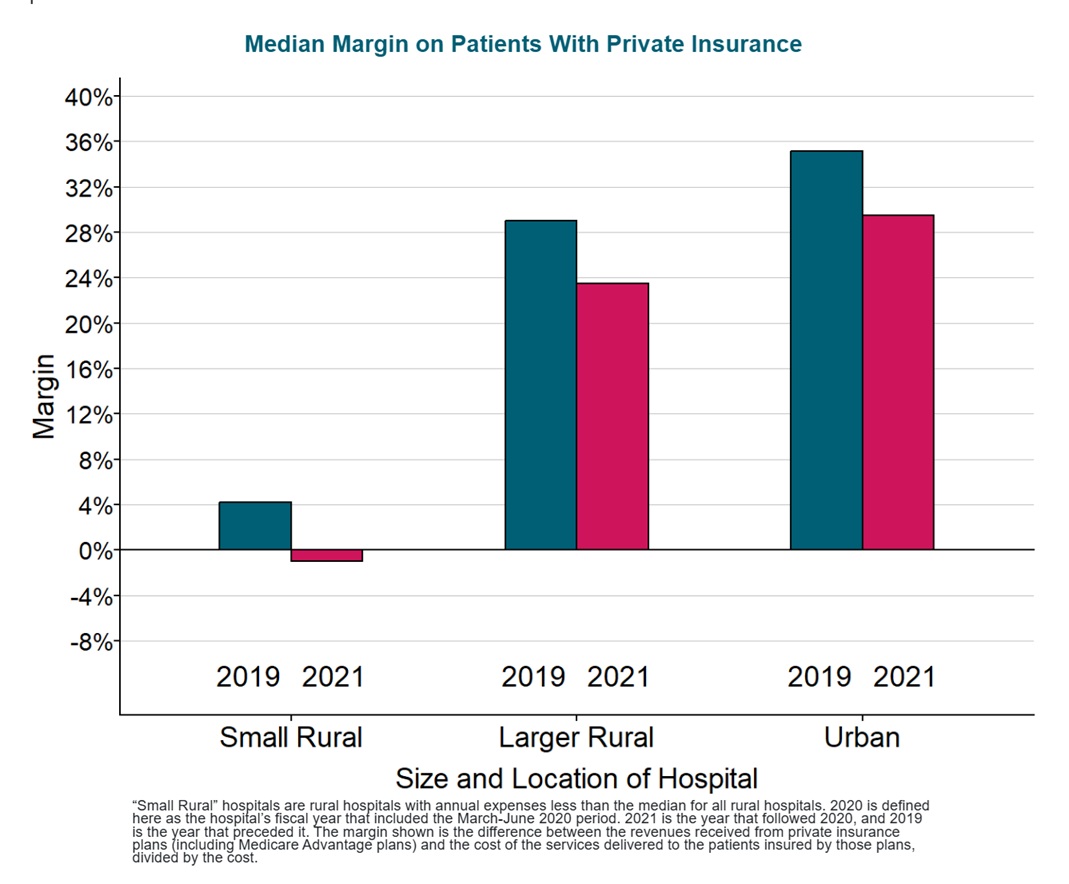
Small rural hospitals lose money on patient services due to inadequate payments from private insurance plans. Whereas urban hospitals and larger rural hospitals make large profits on services to patients with private insurance. Most hospitals, regardless of their size, lose money on Medicaid and uninsured patients. Large hospitals can offset these losses with the profits they make on patients who have private insurance. Due to the traffic and lack of insurance, small rural hospitals can not.
Margins on Services to Patients with Medicare, Medicaid, and Private Insurance
Many small rural hospitals remain open only because they receive significant supplemental funding from state grants or local taxes. In some states, state governments provide grants reducing or eliminating losses at small rural hospitals. There is little or no such assistance in other states. Some small rural hospitals are organized as public hospital districts, and residents of these communities’ tax themselves to offset under-payments by private health plans and Medicaid. There is no guarantee these hospitals can continue receiving these large amounts of revenue in the future, and without them, the hospitals would likely be forced to close.
Contributions of Patient Services and Other Revenues to Total Margins at Closed and Open Small Rural Hospitals

The Impact of the Pandemic on Rural Hospitals
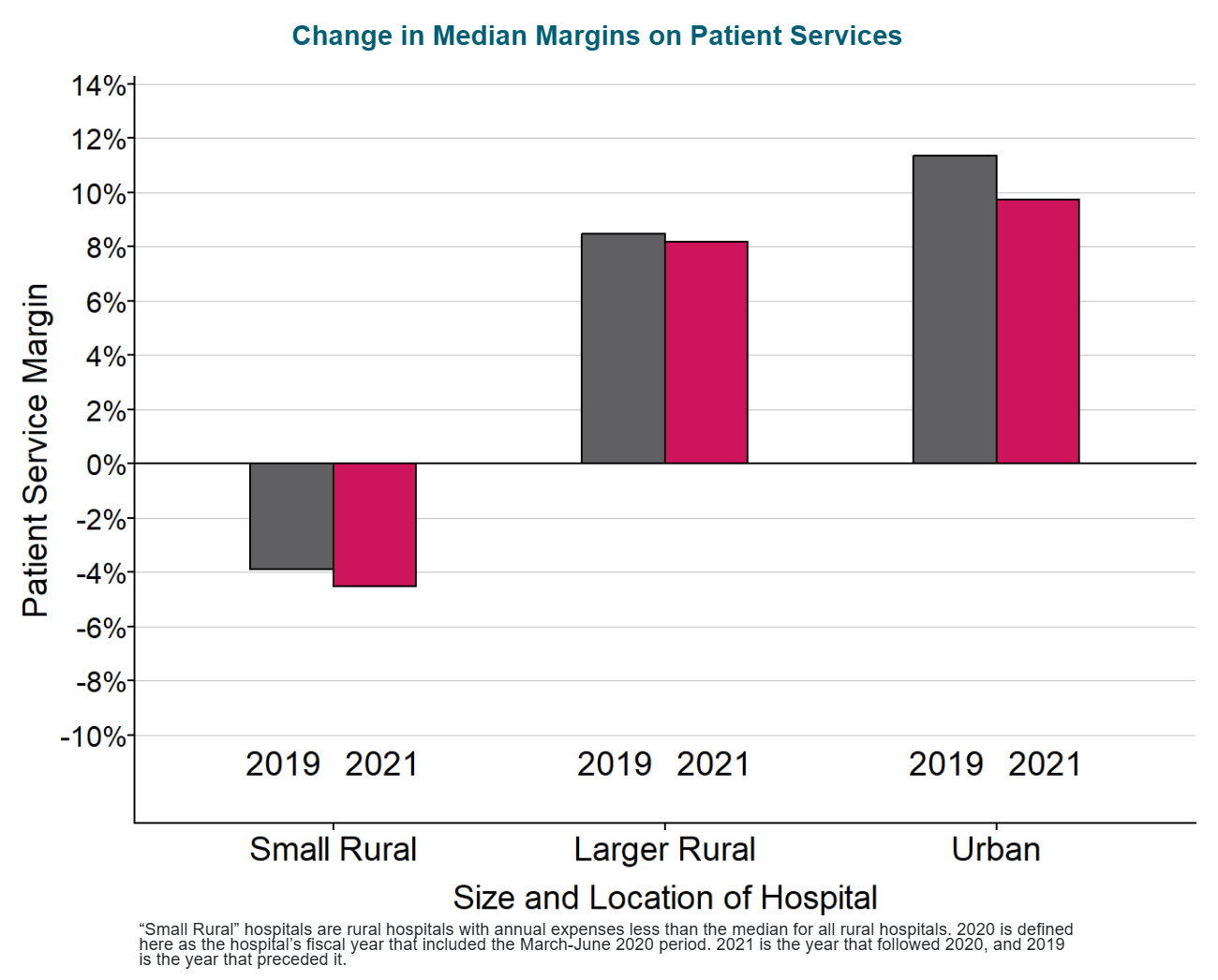
The primary reason overall patient service margins at rural hospitals decreased during the pandemic was higher losses on patients insured by private health plans (including Medicare Advantage plans). The losses on patients insured by private health plans hurt the smallest rural hospitals the most because they were already receiving low payments from private payers prior to the pandemic. Although hospitals of all sizes experienced lower margins during the pandemic on services to patients with private health insurance, the reductions meant that most small rural hospitals lost money providing services to these patients.
Federal assistance enabled small rural hospitals to continue operating during the pandemic. Because the assistance has ended, many hospitals could be forced to close. Despite the higher losses on patient services they experienced, only a few rural hospitals closed during the pandemic because of the special federal funding made available. Most rural hospitals received significant amounts of federal aid enabling them to continue operating. However, this federal assistance was only temporary. The losses on patient services will likely continue or worsen because of the higher costs that rural hospitals are now facing, and without the extra federal assistance, many hospitals will be at risk of closing.
The Problems with Current Payment Methods Summation
Standard payments for hospital services are not large enough to cover the higher cost of delivering services in small rural communities. The average cost of an emergency room visit, inpatient day, laboratory test, imaging study, and primary care visit is inherently higher in small rural hospitals and clinics than at larger hospitals because there is a minimum level of staffing and equipment required to deliver each of these services regardless of how many patients need to use them.
For example, a hospital Emergency Department has to have at least one physician available around the clock in order to respond to injuries and medical emergencies quickly and effectively, regardless of how many patients actually visit the ED. A smaller community will have fewer ED visits, but the cost of the ED will be the same, so the average cost per visit will be higher. Consequently, fees that are high enough to cover the average cost per service at larger hospitals will fail to cover the costs of the same services at small hospitals. Many private health plans pay small rural hospitals less than they pay larger hospitals for the same services, even though the cost per service at the smaller hospitals is inherently higher.
Critical Access Hospital status reduces a small rural hospital’s losses only on services to Original Medicare beneficiaries, and it makes services less affordable for the patients. Most small rural hospitals are classified as Critical Access Hospitals. This enables them to receive cost-based payment for patients with Original Medicare and some Medicaid programs. This results in higher payments for Original Medicare patients than the hospital would otherwise receive. However, it does nothing to reduce losses on uninsured patients and those with other types of insurance, including patients with a Medicare Advantage plan. Medicare rules also requires patients to pay higher cost-sharing amounts in order to receive services at Critical Access Hospitals than at other hospitals. The higher payments for the hospital can have negative financial impacts on its patients.
Current methods of payment penalize hospitals for efforts to improve the health of rural residents. If community residents are healthier and need fewer ED visits and other services, the hospital’s revenues decrease. The cost of maintaining the essential services will not change, thereby increasing financial losses at the hospital. The same problem occurs under Medicare’s cost-based payment system for Critical Access Hospitals. Medicare’s share of the hospital’s costs decreases if Medicare beneficiaries need fewer services.
Health Insurance Coverage and Cost – RHI hub
Individuals without health insurance have less access to healthcare services. According to Geographic Variation in Health Insurance Coverage: United States, 2022, nonmetropolitan children and adults under 65 were more likely than their metropolitan peers to be uninsured.
Our local rural hospital in Washington State has to cover a lot of the uninsured, but it is in better shape than the even smaller hospital to the west of us. Another issue working against rural hospitals is the lack of human capital. This hits us two ways. It makes skilled workers more expensive, so it is harder to recruit doctors, nurses and other staff. It also makes it harder to find good people to serve on the board and as administrators.
Kalesburg: An earlier commentaries of mine:
Millions of Americans No Longer Have Hospital Care in Their Community
Rural Hospitals Financial Losses, Closures, and Revenue
I posted on this issue many times before. Here are a couple of the commentaries. There are more you can find on Angry Bear if you use the search function on the title page.