Republicans say VA patients can get equivalent private-sector care anywhere in the U.S.
Here’s a 50-state reality check of whether that is true or not as discussed by Veterans Healthcare Advocate Suzanne Gordon
The Illusion of Choice
Republicans say that VA patients can get equivalent private-sector care anywhere in the U.S. Here’s a 50-state reality check.
At his confirmation hearing in January of 2025, Secretary of Veterans Affairs Doug Collins, a former congressman from Georgia, assured the Senate Veterans’ Affairs Committee of his commitment to provide specialized, high-quality medical care for the roughly nine million veterans enrolled in the nation’s largest and only truly integrated public health care system, the Veterans Health Administration (VHA).
But Collins, a chaplain in the Air Force Reserve, also explained that his mandate from President Trump is to make it “easier for veterans to get their health care when and where it’s most convenient for them,” by giving them greater choice between in-house and outsourced care. To do this, he planned to lean on the network of 1.7 million private-sector providers who are part of the Veterans Community Care Program (VCCP), created by the VA MISSION Act of 2018. Annual reimbursement of these non-VHA doctors, therapists, hospitals, and clinics now costs the federal government more than $30 billion per year, nearly one-third of the VA’s entire direct care budget.
Collins’s proposed budget for fiscal year 2026 calls for a 50 percent increase in discretionary VHA spending on private care and a 17 percent reduction in discretionary direct care funding. (The overall proposed budget for VA medical services increases, but only because of a large boost in the mandatory Toxic Exposures Fund, which provides health services for veterans exposed to burn pits and environmental exposures. All other diagnoses not in the TEF authorizing legislation would fall under the reduced discretionary budget, and even adding mandatory spending, private care is poised to increase at nearly twice the rate of VA direct care.) And Collins has taken other steps consistent with the goal of downsizing direct service provision and boosting the VHA’s reliance on outside vendors.
Republicans in Congress routinely assert that veterans can easily find better and faster treatment outside the VHA. That’s because they assume that we have enough hospitals, primary care providers, specialty physicians, and mental health therapists to care for the country’s current patient load of 330 million nonveteran Americans, let alone nine million more veterans.
To test the accuracy of these claims, the Veterans Healthcare Policy Institute (VHPI) partnered with the Prospect on a survey of the U.S. health care landscape in all 50 states. State by state, we looked at the data on the current available supply of primary care providers, mental health professionals, and hospitals, particularly in the rural (and remote rural) areas where about one-quarter of all veterans, or about 4.7 million, reside, with 2.8 million of them enrolled in the VHA.
This analysis reveals a system that cannot provide even basic medical and mental health services to nonveteran patients. Hundreds of hospitals in America’s rural counties and underserved areas have curtailed critical services or closed entirely. And thousands of counties across America are experiencing significant health provider shortages, according to federal data.
The dramatic shortfall in capacity in our nation’s health system will get even worse with the passage of President Trump’s One Big Beautiful Bill Act. On top of unilaterally imposed cuts that are already crippling the nation’s academic medical centers, the law, signed on July 4, will impose over a trillion dollars of cuts to Medicaid and the Affordable Care Act. Around 17 million people are expected to lose their health insurance due to Trump’s policies, guaranteeing increased uncompensated care at emergency rooms. States will also have less money to fund their Medicaid programs. All of this will lead to additional hospital closures and more shortages of health care personnel.
Yet, at precisely this moment, President Trump, VA Secretary Collins, and Republicans in Congress also want to send more veteran patients into an already troubled private-sector system, while depleting that system of the resources necessary to absorb this extra load. The idea that this will work well is shaped more by ideology than reality.
One longtime VA expert observed: “Imagining that you can add more complex VA patients into a private-sector system that will be reeling from, and contracting because of, funding cuts is nothing short of delusional.”
A Case Study in Coordinated Care
“Will Smith,” whom I have given a pseudonym for reasons of medical privacy, is a 75-year-old Army vet who fought in the Vietnam War. Because of his combat exposure, Smith struggled with post-traumatic stress disorder (PTSD) after leaving the military. Thanks to VHA therapists and many years of peer group support, he no longer abuses alcohol or prescription drugs.
Like other Vietnam vets exposed to Agent Orange, he has diabetes, which has led to chronic heart problems and kidney disease. Because of the heavy backpacks he carried “in country,” he also suffers from osteoarthritis in his hips and knees, severely limiting his mobility. To get around, he depends on an electric wheelchair provided by the VA. He takes 18 different drugs (all delivered free of charge) to help control multiple “co-morbidities.”
Smith’s primary care physician (who chose to remain anonymous, because in the current environment, saying anything good about a system the doctor’s bosses want to close could get the doctor fired) is responsible for coordinating with numerous specialty providers at the large VA medical center where Smith gets his care. The PCP consults regularly with Smith’s cardiologist, pulmonologist, nephrologist, and everyone else dealing with his physical and mental health problems, which have included suicidal ideation.
Smith’s Patient Aligned Care Team includes a medical resident who is training at the VA, like tens of thousands around the country. An RN, a licensed vocational nurse, and a medical service assistant—all of whom have known Smith for years—help make sure that he schedules and shows up for his appointments. A clinical pharmacist monitors Smith’s use of medications to ensure that he’s taking his pills correctly: some with food, some in the morning and not at night.
More than 89 percent of counties in the United States are officially designated Health Professional Shortage Areas.
Smith’s doctor schedules 60-minute, in-person visits with Smith every three months and a telehealth appointment every six weeks. In between these consultations, Smith’s weight and blood pressure are checked daily through a VA telemonitoring service, which sends alerts to his care team if worrisome changes are detected. There is no patient fee for this service. If Smith needs equipment essential to facilitate his care, like a laptop, iPad, or smartphone, the VA also provides it, free of charge.
The VA’s integrated health service provides Smith with acupuncture and chiropractic sessions to help him manage chronic pain. When able, Smith tries to attend a chair yoga class, one of many such offerings that include popular mindfulness meditation sessions.
Our pseudonymous Will Smith is not an outlier, in terms of his complex care needs. As a 2016 RAND report confirmed, “VA providers are likely to be treating a sicker population with more chronic conditions, such as cancer, diabetes, and chronic obstructive pulmonary disease (COPD), than the population expected by civilian providers.”
A 2021 report from Brown University’s Cost of War Project underscored that the open-ended global war on terror has produced the most disabled cohort of veterans in American history. Nearly two million veterans of post-9/11 wars have paid a heavy price for their military duty. About 40 percent have a service-related disability, compared to 25 percent of all veterans of World War II, the conflicts in Korea and Vietnam, and the first Gulf War, who came back injured in some form.
As congressional hearings and debate before passage of the Promise to Address Comprehensive Toxics (PACT) Act revealed, hundreds of thousands suffer from long-term illnesses stemming from exposure to burn pits in the Middle East or poisoned groundwater at U.S. military bases around the country , like Camp Le j eune.
Veterans who rely on the VA for health care are also more economically disadvantaged than most other patients in the U.S., with the exception of Medicaid recipients. As one study found, they tend to be less educated and have lower household incomes. According to VA data, about 50 percent of veterans have a personal annual income of $50,000 or less; less than 5 percent, mainly former officers, have an annual income of $200,000 or more.
Whether they live in urban or rural America, veterans steered away from the VA through expanded outsourcing will become “customers” of private health care networks that are quite different from what they are used to. As the Commonwealth Fund points out, the health outcomes in the non-VA system include one of the industrialized world’s highest suicide rates and the highest rate of avoidable mortality, as well as fewer hospital beds, physician visits, and even practicing doctors than other equivalent countries have.
Access Problems
Although access to primary care is widely recognized as central to “health equity and care access,” more than 89 percent of counties in the United States are officially designated primary care Health Professional Shortage Areas (HPSAs). About 80 million Americans, nearly one-quarter of the total population, live in areas without enough primary care providers.
As a result, almost all of America’s rural counties are at significant risk of poorer health, with residents of Alabama, Georgia, Mississippi, New Mexico, and Texas at even greater risk. Rural America contains about 25 percent of the veteran population.
The numbers are staggering. Arizona will face a shortage of 8,280 physicians by 2030, according to the Cicero Institute; Texas will need 20,420 more physicians by that year. Many of Louisiana’s parishes have only one or two full-time primary care physicians, and nearly half of Kentucky’s primary care physicians work in just two of its 120 counties. Fifty-two of Montana’s 56 counties have serious shortages of primary care providers; every county in Idaho, South Dakota, and Wyoming has severe shortages of mental health providers. In rural areas of Colorado east of Denver, there is only one primary care physician for every 5,636 residents.
Long-standing nationwide shortages of primary care providers make it difficult for primary care practices to take on new patients. In 2023, for example, the VA announced a “historic public-private partnership” between the VA and the University of Pennsylvania Health System. The collaboration was intended to try to replace the closure of VA facilities in Philadelphia and Coatesville, which served thousands of patients.
So, two years ago, the Prospect played secret shopper to assess the availability of primary care appointments for new patients at Penn Med. The system’s primary care website revealed that a significant number of affiliated practices were closed to new patients. We then called a sample of the primary care practices whose patient panels were listed as still open, only to discover that to get a first appointment would take four or five months.
There are, of course, wait times at the VA. We know what they are, because the VA actually calculates and publicly posts them.
One of the only ways to find equivalent information about private-sector wait times is to actually wait for the survey published periodically by the private consulting company AMN Healthcare (formerly Merritt Hawkins). Even this data is severely limited. AMN collects wait time data from only six medical specialties—cardiology, family practice, orthopedic surgeons, obstetrics/gynecology, dermatology, and gastroenterology—in only 15 different major metropolitan areas.
The data is not reassuring. AMN’s 2025 survey found that, since 2022, the average wait time for physician appointments increased by 19 percent, with the average time for an appointment at 31 days. The average wait for an appointment with a family practice physician is 23.5 days with a high of 207; for a cardiologist, the wait could be on average 32.7 days, with a high of 175 days. A woman could spend on average 41.8 days, or a high of 231 days, waiting for an ob/gyn appointment. Someone worried about a suspicious blotch on their face could wait up to 291 days to have a dermatologist tell them if it was malignant.
We can expect these manpower shortages and wait times to skyrocket in the next decade, due in part to the aging of the physician workforce. Physicians aged 65 or older make up 20 percent of the clinical physician workforce, and those between ages 55 and 64 are 22 percent. A significant number of physicians, then, will reach retirement age within the next decade.
Unless current conditions change, the Association of American Medical Colleges (AAMC) reports that by 2036, the U.S. will face a shortage of between 20,200 and 40,400 primary care physicians, between 10,100 and 19,900 physicians for surgical specialties, and potentially 5,500 physicians for medical specialties. A 2020 study from several researchers is even more stark: The U.S. shortage in physicians of all kinds will hit 139,160 by 2030.
Mental Health Shortages
When it comes to care for mental health conditions, which 41 percent of the veteran population struggle with, non-VA patient access is already very limited, and that’s an understatement.
In most states, only a handful of counties have even a minimal capacity to deal with nonveterans’ mental health issues, making it hard to imagine that the private-sector system could address the complex mental health conditions of veterans like Will Smith.
In the United States, 123 million people, over one-third of the population, live in a Mental Health Professional Shortage Area. In rural counties, 81 percent do not have a single psychiatric nurse practitioner and 65 percent do not have a single psychiatrist. This may help explain why the suicide rate in rural communities is between 18.3 and 20.5 per 100,000 residents, about 50 percent higher than the rate in urban areas.
Americans with low incomes, and not coincidentally more mental health and substance abuse problems than those in the general population, have even more trouble finding needed care. According to a report from the Medicaid and CHIP Payment and Access Commission (MACPAC), 50 percent of Medicaid enrollees with a serious mental illness are unable to access care, because only about one-third of psychiatrists accept new Medicaid patients.
The aging of the physician workforce means that America needs tens of thousands of new doctors in the next decade.
Even in those urban areas that seem to be well stocked with licensed mental health professionals, 6 in 10 psychologists may not accept new patients, and one-third of psychologists and 45 percent of psychiatrists may not accept insurance of any kind. This means that even patients with good insurance may be unable to get mental health treatment unless they can pay for it out of pocket.
The cost of mental health evaluations and treatment can vary enormously depending on the area of the country, from $65 to as much as $250 per session. The Prospect inquired about how much it would cost for a session of cognitive behavioral therapy, a gold-standard evidence- based treatment that is widely used at the VA in treating PTSD, insomnia, and many other problems. We found that therapists in the Bay Area could charge between $235 and $500 an hour. Almost no one we queried would accept health insurance for CBT treatment. Given the low incomes of most VA patients, they would be out of luck if the VA became just another insurance company.
If a veteran needs psychiatric hospitalization outside of the VA, they may find themselves similarly out of luck. Closures of VA psychiatric inpatient beds are reportedly a problem in some facilities. Along with increasing hospital closures guaranteed by Medicaid and other health care funding cuts, this will pit veterans and nonveterans in a no-win contest for an already inadequate number of psychiatric beds throughout the U.S.
According to a recent report by the American Psychiatric Association, the number of beds available to acutely ill psychiatric patients has dropped significantly in the past 60 years. Patients having an acute mental health crisis can be forced to languish on a gurney in an emergency department hallway, sometimes for several days, or in the worst-case scenarios end up homeless or in jail. Prisons too often become the mental health patient warehouse of last resort.
Rural Hospital Closings
Even before federal cuts of $1.042 trillion from the Medicaid program, the situation for hospitals in rural America was dire. The Center for Healthcare Quality and Payment Reform (CHQPR) notes that in the last decade, over 100 rural hospitals have closed. Since 2005, Texas has lost 25 rural hospitals, the most in the nation, and Tennessee has lost 15.
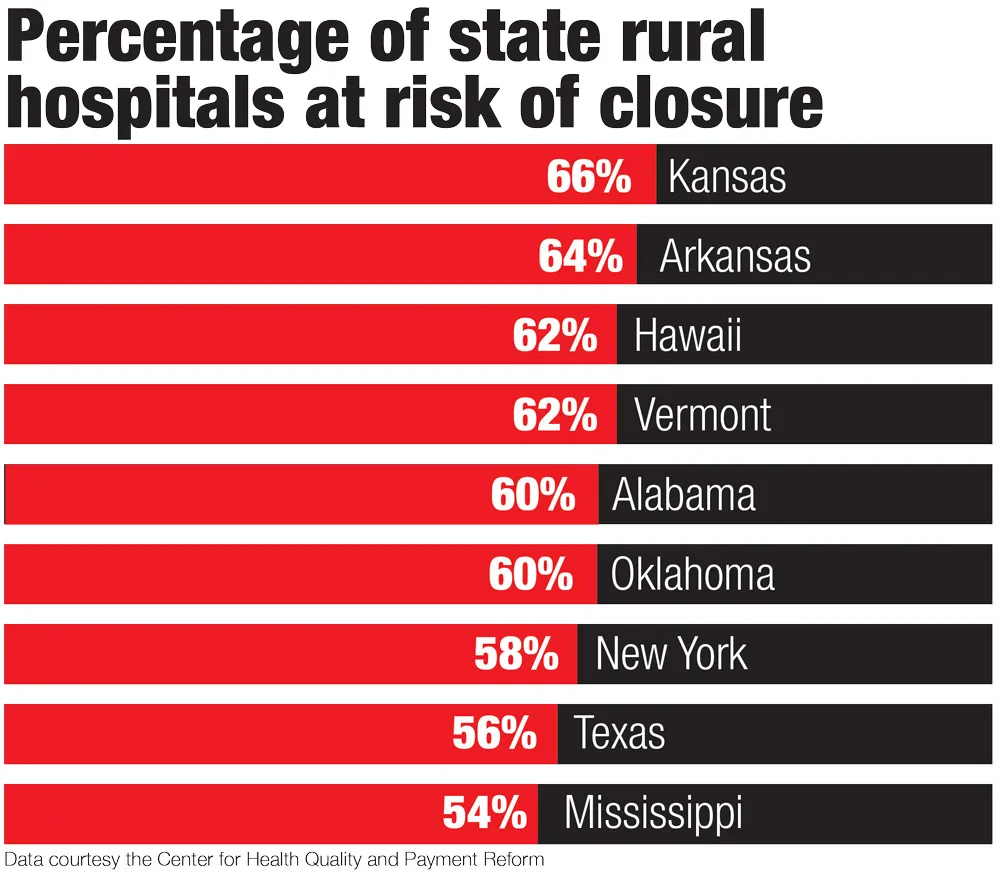
The CHQPR report estimates that more than 700 rural hospitals, one-third of all rural hospitals in the United States, are at risk of closing. In Arkansas (64 percent), Hawaii (62 percent), Vermont (62 percent), Alabama (60 percent), Oklahoma (60 percent), New York (58 percent), Texas (56 percent), and Mississippi (54 percent), at least half of all rural hospitals are at risk. Over 90 percent of rural hospitals in Florida report operating losses, along with 83 percent of rural hospitals in Wyoming.
Rural hospitals that have yet to close are cutting back services. According to a report from health care research group Chartis, “293 rural hospitals stopped offering OB services between 2011 and 2023, while 424 ceased chemotherapy services between 2014 and 2023.” Two-thirds of all rural hospitals in Oklahoma cut services in the last year; 60 percent of rural hospitals in Mississippi cut services.
In July 2025, Becker’s Hospital Review noted that 18 hospitals and emergency departments had closed this year alone. Hospitals and emergency departments in Alabama, Pennsylvania, Texas, Ohio, Missouri, Maine, New York, Florida, Oklahoma, and Washington, D.C., were shuttered.
This is all before the deep Medicaid cuts contained in the Trump budget law. Due to those cuts, the National Rural Health Association (NRHA) estimates that rural hospitals will lose almost $70 billion over the next ten years. A $50 billion rural hospital fund embedded in the law cannot cover the damage to an already fragile system, and the NRHA predicts many hospitals will close. One, in Curtis, Nebraska, population 900, already has, citing the looming Medicaid cuts.
Georgia and Kansas
The Chartis report on the state of rural health care specifically highlighted the plight of rural veterans: “Rural hospital closures and declining access to community care could potentially hinder the intended benefits of policies such as the MISSION Act.”
That is in fact what is happening in two of the states surveyed in our report: Georgia, whose former representative Doug Collins is now VA secretary, and Kansas, whose Republican senator Jerry Moran serves as chairman of the Senate Committee on Veterans’ Affairs.
If Georgia’s 339,000 veterans enrolled in VA coverage are pushed into the private sector, they will enter a health care market where the physician-to-patient ratio is 23 percent worse than the national average. Overall, Georgia ranks in the bottom half of states for primary care and physician availability. A 2020 study of primary care shortages found that many residents of Georgia are extremely vulnerable to poor health outcomes because they live in poverty, which leads to more serious medical conditions that often go untreated.
Of Georgia’s 159 counties, nine have partial shortages of primary care providers, while 134 have severe shortages. Only 16 register no PCP shortages. Even in many of the counties without shortages, primary care practices can be overburdened and/or closed to new patients. Plus, Georgia will be short 8,012 physicians by 2030.
Most Americans have fewer and fewer health care choices, and are about to pay more for even less.
The mental health situation in Georgia is even bleaker. Of Georgia’s 159 counties, 152 have a severe shortage of mental health providers. Only six counties register no shortages; however, in these counties many mental health professionals may not be open for business to patients who can’t pay out of pocket. KFF estimates that 33.9 percent of Georgia residents report symptoms of anxiety or depression, which may be untreated because of shortages of mental health professionals. The rate of deaths from drug overdoses in Georgia has doubled over the past ten years, and its suicide rates are higher than the national average.
Since 2015, Georgia has lost nine rural hospitals, and another 20, representing 28 percent of the state’s rural hospitals, are at risk of closure, with 13 percent at immediate risk.
When we turn to Jerry Moran’s Kansas, the situation is all too familiar. Should more of the 86,000 Kansas veterans enrolled in the VA move into the private sector, they will find that 71 of the state’s 105 counties have severe shortages of primary care providers. Even in the 34 counties that do not register shortages, many practices may be overburdened and/or closed to new patients. According to one report, the “shortage of Kansas doctors has major impact on the health of its citizens. Rural Kansans face the prospect of more chronic disease, greater morbidity from their chronic conditions, and a higher mortality rate than their urban counterparts. The lack of primary care physicians compounds the impact this has on individuals and communities.”
Only four of Kansas’s 105 counties, all near Topeka and Kansas City, don’t register severe shortages of mental health professionals. There are only 314 licensed psychologists and only 300 psychiatrists to serve the state’s nearly three million residents. As we’ve seen, many may not accept new patients, or may restrict new patients to those who can pay out of pocket. The situation is also compounded by the fact that 6 out of 10 Kansas psychiatrists are over 55, thus nearing retirement.
This is one of the reasons why the more than 37 percent of Kansas residents who suffer from depression or anxiety disorder have trouble accessing treatment. The rate of deaths due to drug overdoses has more than tripled in the last decade, and the suicide rate is also higher than the national average.
The crisis in the state’s hospitals is one of the worst in the nation. Kansas, Chartis reports, is one of seven states tied for the hospitals with the greatest loss of inpatient care in the country, and it also ties with another four when it comes to states with the highest number of vulnerable hospitals in the country. Of Kansas’s 100 rural hospitals, 89 have lost services, 66 are at risk of closing, and 29 are at risk of immediate closure. Kansas also has the honor of being one of the three states in the nation with the highest loss of rural OB units in the country.
A Chaotic Restructuring
During his first six months on the job, Collins ordered the illegal mass firing of 2,400 VA probationary employees. He developed a plan to cut 15 percent of his agency’s workforce by late 2025, and canceled hundreds of contracts with researchers whose work also supports patient care. He ended remote work arrangements and ordered mental health care providers to report back to facilities not properly set up for telehealth work. This chaotic restructuring, driven by the Trump-created Department of Government Efficiency, has led to widespread workplace disruption, rapidly cratering morale, and uncertainty for thousands of career employees at the VA.
If VA services or facilities are cut around the country, shortages of primary care providers, medical specialists, and mental health professionals will increase. That’s because the VA plays a pivotal but largely unrecognized role in our system of training health care professionals, through educational partnerships with 90 percent of U.S. medical schools. Congress allocates funding so that the VA can train about 75,000 medical students and residents at the VA every year. The Association of American Medical Colleges has called the VA an “irreplaceable component of the U.S. medical education and research enterprise.”
The VA also trains 60 other categories of health care professionals, including nurses, and optometrists, and pharmacists, and psychologists. The VA, which is the single largest employer of psychologists in the country, trains 1 in 5 of the nations’ future Ph.D.s in psychology. The continued existence of these professional training programs depends, however, on the VA having enough patients to provide trainees with enough of a diversity of clinical experiences, as well as enough expert staff to educate and monitor trainees.
If too many patients are sent out of the system or there aren’t enough staff to teach trainees, training programs won’t be accredited and will end. Former VA undersecretary for health Kenneth W. Kizer believes this could “have widespread effects on the provision of care in the United States, and could exacerbate health care professional shortages.”
But when veterans groups, VA patients and their families, or caregivers protested these changes, Republicans in Congress dismissed their concerns. According to House Veterans’ Affairs Committee chairman Mike Bost (R-IL), the “VA bureaucracy” itself “poses a greater danger to the health of our veterans than the illnesses they seek treatment for.”
Bost and other Republicans in Congress have introduced multiple bills that would greatly expand the outsourcing authorized by the MISSION Act seven years ago. For example, Sens. Marsha Blackburn (R-TN), Tim Sheehy (R-MT), Roger Wicker (R-MS), and Tommy Tuberville (R-AL) have sponsored the Veterans Health Care Freedom Act, to “provide veterans with greater autonomy to access the care they need.” This legislation goes beyond recent patient referral rule changes made by Collins. It would allow veterans to make appointments with private-sector providers in the VCCP without any prior consultation with or authorization from their in-house provider.
Other red-state Republicans, who also represent many veterans in rural areas, have jumped on the bandwagon. Earlier this year, Sen. Kevin Cramer (R-ND) joined Sheehy as a co-sponsor of the Critical Access for Veterans Care Act. Their bill would steer more veterans toward “health care services at their local rural hospital or clinic under the VCCP.”
That movement of patients into private-sector care, along with the significant funding resources being taken out of the system by Medicaid and Affordable Care Act cuts, will push a system on the brink of collapse at both ends.
Conclusion
The nation’s nine million veterans enrolled in the VA health care system have been largely sheltered from the everyday realities of a deeply flawed private-sector market. They may not like having to wait for an appointment or having to travel an hour to a VA community-based outpatient clinic. But once enrolled in the VHA, veterans receive care that is of higher quality, with shorter wait times, than non-VA patients receive. While the average American, if they are insured, may have access to medical treatment, few have ever experienced the kind of wraparound services that are routinely provided to veterans like Will Smith.
In 2016, conservative writer and co-chair of the Koch brothers–funded “Fixing Veterans’ Healthcare Task Force” Avik Roy argued in The New York Times that “veterans should enjoy the same health care options as all Americans.” He claimed that ordinary Americans were far better off, because they could take advantage of a “vast array of private health care and coverage options that are denied” to veterans. As our state analysis demonstrates, nothing could be further from the truth. Most Americans have fewer and fewer health care choices, and are about to pay more for even less. And if VA privatization continues, veterans like Will Smith will lose the one option they say they most value: a health care system in which Americans have invested for over a century and that has more than fulfilled its promise to care for those who have borne the battle.
The Illusion of Choice – The American Prospect, August 4, 2025
“The idea that this will work well is shaped more by ideology than reality.”
A polite way of saying they’re lying.
Isn’t the official line that at least we don’t ration health care the way they do in government provided health care countries. I knew that it’s sometimes hard to find a doctor with an open practice, but those numbers are astounding. I knew capitalism was bad, but I hadn’t realized how bad.