What Defenses and Practices Mostly Worked During the Covid-19 Pandemic
Another add-on from yesterday as to why people should take precautionary actions when confronted with a pandemic such as Covid-19, the flu, or other contagions. There was much resistance to taking precautionary measures under the guise of a freedom to do what they wish to do mentality. Thousands of people paid with their lives after contracting Covid-19. Many of them decided they did not need to take any precautionary actions.
Masks, social distancing and vaccinations worked
by Merrill Goozner
GoozNews
Under U.S. law, states have the primary responsibility for protecting public health. The Centers for Disease Control and Prevention can make recommendations and give grants for specific programs, but the federal government allows state and local health departments to determine their own priorities.
The COVID-19 pandemic exposed the weakness of this decentralized approach. Within a month of then-president Donald Trump declaring a national emergency on March 13, 2020, the CDC (after some initial waffling) recommended everyone wear masks and engage in social distancing when out in public. By November, 37 states had adopted mask mandates or required people stay separated when in public places.
The federal government never officially recommended states adopt stay-at-home policies. But within three months of the outbreak, 42 states had issued such orders for “non-essential” businesses. That spring, over three-quarters of U.S. public schools switched to remote learning, a number that rose to 80% by fall. Many businesses (especially restaurants) shut down or switched to take-out only. For millions of workers with desk jobs, work-at-home became a way of life.
However, enforcement of all those policies was largely non-existent. Widespread resistance emerged within months. Ditto for vaccine mandates once the two-shot regimen became widely available in the fall of 2021.
Resistance began at the top. When, on September 26, 2020, then-president Donald Trump held an outdoor ceremony to announce Amy Coney Barrett’s nomination to the Supreme Court, everyone sat cheek-by-jowl in the Rose Garden. Only a few wore masks. During the first debate on September 29th, Trump mocked Joe Biden: “I don’t wear a mask like him. Every time you see him, he’s got a mask.” A day later, Trump, the First Lady and senior advisor Hope Hicks tested positive for COVID, forcing the president to enter Walter Reed Hospital for a three-day stay.
Numerous businesses that had been deemed non-essential challenged the shut-down orders. Court suits were filed in Wisconsin, Pennsylvania, Arizona and New Mexico. Trump encouraged businesses to stay open saying, “We can’t have a cure that’s worse than the disease.”
During 2021, after the new COVID-19 vaccine proved remarkably effective at reducing the severity of the disease, President Biden required vaccinations for federal employees and contractors. He proposed all businesses with over 100 employees either do the same or test their employees weekly. Governors in GOP-run states declared the move “terrifying” and a “power grab,” which helped stoke resistance among a small but vocal minority of the population. The U.S. vaccination rate remains in the lower tier among advanced industrial nations.
51 petri dishes worth studying
In other words, the U.S. failed to mount an effective national response to COVID-19. Instead, states and the District of Columbia adopted a patchwork quilt of requirements and recommendations. Even where restrictions and mandates were in place, enforcement was mostly a non-event with states relying on voluntary compliance.
Still, some of those measures may have had a huge impact on reducing disease incidence and mortality during the pandemic. Given the uneven nature of their adoption between states, the U.S. became the ideal place for studying the impact of various interventions.
The challenge was taken up by Christopher Ruhm, a professor of public policy and economics at the University of Virginia. Ruhm’s study, released today on the JAMA Health Forum website, shows states that adopted the strictest COVID-protection policies had significantly lower death rates than states that had the least restrictive policies. He calculates that if every state had adopted the policies enacted by the ten most restrictive states, anywhere from 118,000 to 148,000 additional lives would have been saved between July 2020 and June 2022, a period when the pandemic was raging in almost every state in the nation.
On the other hand, if every state had followed the path taken by the ten least restrictive states – a move pushed by conservative scholars associated with the Great Barrington Declaration, which encouraged the pursuit of “herd immunity” to curb COVID – an additional 150,000 to 200,000 lives would have been lost. There was an estimated 25% to 48% difference in mortality rates between the most restrictive and least restrictive states.
“Strong COVID-19 restrictions saved lives,” Ruhm concluded. “The death toll was probably considerably higher than it would otherwise have been in states that resisted imposing these restrictions, banned their use, or implemented them for only relatively short periods of time.”
Ruhm, who served as a senior economist for the Council on Economic Advisers during the Clinton administration, excluded data from the first four months of the pandemic. During that initial phase, half of all COVID cases and deaths took place in just four northeastern states with the most exposure to foreign travelers. In addition, intervention measures in most states were just ramping up as the scientific understanding of how the disease spread evolved.
The study evaluated the effects of 10 separate restrictions and individual behaviors enacted in that first year. The restrictions included requirements and/or restrictions for both masking and vaccinations; self-reported masking adherence; stay-at-home orders; closures of restaurants, bars, theaters, schools and other leisure time activities; and restrictions on public gatherings.
Most v. least restrictive states
Ruhm created a composite score for each state and then ranked them from “most restrictive” to “least restrictive.” The ten states with the most restrictive policies were (in alphabetical order): California, Connecticut, the District of Columbia, Delaware, Hawaii, Illinois, New Mexico, New York, Oregon and Washington. The ten states with the least restrictive policies were Florida, Georgia, Idaho, Iowa, Oklahoma, South Carolina, South Dakota, Tennessee, Texas and Utah.
He then compared the all-cause mortality rates in those two groups to their pre-COVID rates. Overall, the difference between the two groups was stark. But not all interventions were equally effective. And some weren’t effective at all.
For instance, states that adopted the strictest policies on masking and social distancing saw the smallest rise in all-cause mortality during the pandemic. States that resisted those policies had the biggest increases. Vaccine mandates were also highly effective in reducing death rates as would be expected given the vaccine’s effectiveness in reducing disease severity.
Picture
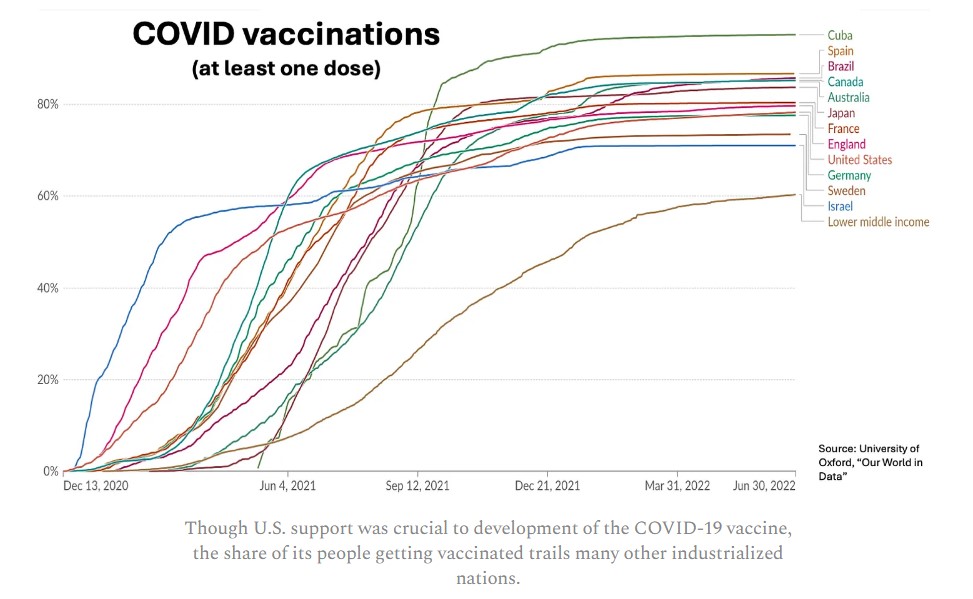
Though U.S. support was crucial to development of the COVID-19 vaccine, the share of its people getting vaccinated trails many other industrialized nations.
Major limitations on social, business and school activities, on the other hand, did not reduce the death rates. But neither did they raise them, a claim that has been made by some opponents of restrictions who suggest limits on access to health care, among other things, cost lives.
In an interview this week, Ruhm told me that some of the study’s peer reviewers questioned that finding. He wishes everyone would lower their defenses and begin learning from the experience of the past four years, which is now possible if we take a close look at the data.
Some things worked very well; others not so well, he said. “It is clear schools were closed for too long in many places. The costs of that exceeded any benefit. But what is even more frustrating is this notion that overall these restrictions did not work.
“Vaccinations were incredibly important as were masks and social distancing. Maybe we should have realized faster than some (restrictions) were not ideal. There were cases where the balance should have been tilted in different ways. But this notion that these things were just harmful or ineffective? An objective look at the evidence does not support that view. As packages, the states that had stronger restrictions saved hundreds of thousands of lives.”
The next Congress needs to make pandemic preparedness one of its highest priorities. A first step would be establishing a commission that can draw firm conclusions about what worked and what didn’t during the COVID-19 pandemic. It must address flaws in our decentralized response system. And it should provide guidance on what it will take to win broad public acceptance for necessary public health measures, which will save lives during the next pandemic, an inevitability in our warming world.
Odd graph. Many nations and then “lower middle income”. Is that of all the countries on the graph?
Nothing odd about it ~ it details the countries reporting. What makes you think so?
“Major limitations on social, business and school activities, on the other hand, did not reduce the death rates. But neither did they raise them,” In other words, we caused a lot of economic harm for no reason, as the quoted article says. These ineffective measures were imposed by government fiat. And we censored and ostracized those who disagreed. Shame on us twice.
““It is clear schools were closed for too long in many places. The costs of that exceeded any benefit. ” – I think we should have realized this very early (March 2020) based on who was dying from Covid in Europe. We implemented these policies even after the FDA wanted to reopen the schools. The Teachers’ unions pushed the administration to retain the policies. Politics > science.
Vaccines worked. Not perfectly, with some side effects, but they worked. Clearly advisable for anyone at risk of serious illness. Pick an age probably somewhere above 40 or 45, and include the obese, diabetics, those with weak kidneys, other known dangerous comorbidities for strong encouragement for vaccinations. Younger folk probably didn’t need them and they do assume some long term known and unknown risks.
(Side issue: our government should have gone on a national exercise and anti-obesity campaign during Covid. It would have helped national health and blunted one of the most deadliest Covid-comorbidities’ impact.)
Masks? The best data seems to come from the Cochrane study which shows little or no effect. https://www.cochrane.org/CD006207/ARI_do-physical-measures-such-hand-washing-or-wearing-masks-stop-or-slow-down-spread-respiratory-viruses Of course, not everyone agrees. But there it is.
The best data comes from a report which says
???
I didn’t say perfect, or even good. I said “the best data we have”. If that results in little to no evidence, we should say, “we don’t know”. One is left wondering on what basis some people came to accept the opposite belief. I suspect they simply looked around at what was socially acceptable and emulated that. How do you support your beliefs in the absence of evidence?
The study that you have chosen to promote did not attempt to measure if masks control or reduce the source of spread. The study also chose to limit its analysis to only randomly controlled trials of masks and how they impacted receiving and contracting the virus.
The study determined that given these self imposed guidelines, they could make no determination.
This is fine.
But it is deeply ignorant or purposefully misleading to say that this is the best source of info on the effectiveness of mask use.
Just because it is the conclusion you like doesnt mean it is the best info we have.
But you dobget bonus internet irony points for attacking others for your own approach to the issue.
Posting a demand for evidence below an article about the evidence you claim doesnt exist certainly indicates its probably not deep ignorance….
Additionally, the Cochrane (meta)study makes claims about having the “best” data because it surveys only double blind studies. This entirely ignores real life data. A cursory look at results in China and New Zealand shows that policies certainly can reduce the spread.
Gonna’ tell an overweight MAGAt refusing to wear a mask to lose weight
Rolling on the floor laughing my rosy red hindside off
Unfortunately most Americans could use losing weight. Some call it an epidemic of obesity. Stay classy, 10Bears…
A centralized approach? First off, that will NEVER happen. Our federal government is completely incapable or running any centralized agency anywhere close to efficiently. I never took the vaccine, never socially distanced and seldom wore a mask. I did this because I had the common sense to synthesize the data and discern that I was in an extremely low risk category of contracting a severe case of Covid. Low and behold my calculations were correct. As for analyzing which states fared better and owing that to restrictions is a little more complicated than you make it out to be. What was the ratio of high risk to low risk population? What was the elderly per capita population? What was the obesity rate per capita? Pre-existing comorbidities? To just say the states with more restriction did better is telling only a very small portion of the story.
I think I just noticed a rather large flaw in this study. If they excluded the early months of the pandemic, when most of the Covid was concentrated in NY/NJ/CT and CA, doesn’t that undercount the deaths in those states to skew the results and make the other states look worse? I’m going to read the study, but I hope they controlled for different average ages, comorbidity and obesity rates among states. They are different and almost certainly had a differential impact. Another wild card is when, in the course of the pandemic, did a state become “hot”. Meaning we knew more by the end of 2020 than we did in the beginning. How do we control rates of death in states that got Covid early, vs late?
Conclusion
A randomized-trial of community-level mask promotion in rural Bangladesh during the COVID-19 pandemic shows that the intervention increased mask usage and reduced symptomatic SARS-CoV-2 infections, demonstrating that promoting community mask-wearing can improve public health.
Impact of community masking on COVID-19: A cluster-randomized trial in Bangladesh
Impact of intervention on mask use and biological outcomes.
The figure shows the raw means of mask-wearing (left), COVID-19 symptoms (middle), and symptomatic seropositivity (right) in the control and treatment arms. The estimated change in each outcome, confidence intervals, and p values adjust for preregistered covariates (and thus are not computable from the raw values). Individuals who were symptomatic but did not consent to blood collection were dropped from the sample; measured symptomatic seropositivity thus understates the true fraction of the population that was symptomatic seropositive.
Abstract
We conducted a cluster-randomized trial to measure the effect of community-level mask distribution and promotion on symptomatic severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections in rural Bangladesh from November 2020 to April 2021 (N = 600 villages, N = 342,183 adults). We cross-randomized mask type (cloth versus surgical) and promotion strategies at the village and household level. Proper mask-wearing increased from 13.3% in the control group to 42.3% in the intervention arm (adjusted percentage point difference = 0.29; 95% confidence interval = [0.26, 0.31]). The intervention reduced symptomatic seroprevalence (adjusted prevalence ratio = 0.91 [0.82, 1.00]), especially among adults ≥60 years old in villages where surgical masks were distributed (adjusted prevalence ratio = 0.65 [0.45, 0.85]). Mask distribution with promotion was a scalable and effective method to reduce symptomatic SARS-CoV-2 infections.
Looks like the older people get screwed again, heh. Cannon fodder so eveyone else feels good, heh?
Matt
you may have been at low risk for serious disease, but were you at low risk for carrying the disease and infecting others?
thecomments here reflect the difficlty of “educating” people. But a demagogue can dis-educate them very easily.
There would have been no need for “forced” anything if we had leadership capapble of making the case for doing it “voluntarily.” Instead we had leadership telling them it was their right to be stupid…prove they were smarter than the “experts.’
the post itself shows loopholes in “the science,” but “the science” is still the best bet we have if only the science and the government had a reputation for honesty and knowing what they are talking about.
speaking of bets, you understand you are betting your life…and that of someone close to you…and a bet is just that..a guess about how lucky you are.
i made an enemy on AB because I disagreed with him about the “authority” of “science” or the authority of those claiming to be an authority on science, as well as the political and personal-sanity risks of saying other people deserve contempt and should be forced to do what he thinks is best for them and, especially, himself.
but that does not mean i have any more respect for the people who make their decisions based on what the leader of their tribe tells them and their own personality problems that lead them to worship such a leader.
for a different take “The Premonition’ talks about the whole from a point of view that is pretty much the same as mine about group-think versus the insights of someone smart, honest, and experienced.
I can’t guarantee he is right (or that I am right), but it is a point of view worth thinking about along with all the other points of view you are not thinking much about.
author of The Premonition: Michael Lewis