Coronavirus dashboard for June 27: infections -> hospitalizations -> deaths
Coronavirus dashboard for June 27: infections -> hospitalizations -> deaths
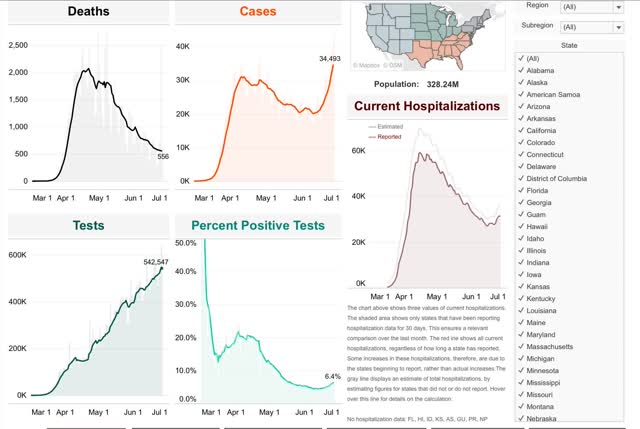
Total US deaths: 125,120, 619 new deathsA quandary over the past month has been why deaths declined so much more than new cases, while cases were declining; and more recently why deaths have continued to decline in the face of soaring new infections.Is it because of better treatments? Changing demographics – e.g., fewer nursing home cases, more younger people? Or is something more even more fundamental with the nature of the virus itself going on? In short, should we expect deaths to continue to decline, or to turn up following the increase in new infections?I am expecting deaths to begin to rise again, imminently.Here’s why: the progression is:
– first, infections increase/decrease
-second, hospitalizations increase/decrease
-finally, deaths increase/decrease.
The problem in the US data has been that hospitalizations have been missing from almost all compilations. That’s because not all States – and most especially, Florida – track hospitalizations.
Conor Kelly, however, *does* track reported hospitalizations from all States which have reported for at least 30 days, which totals roughly 40 States. So if deaths are going to start to increase again, it should first appear in this data. Further, if this is because of the reckless reopening of some States, it should most plainly appear in those regions. With that in mind, here is the data.
Total US hospitalizations bottomed on June 14 at 26,441. In the 12 days since, they have risen by almost 14% to 30,065:
One benefit of Conor Kelly’s compilation is that it allows users to generate customized regions of States. So, for example, here is the data for the East Coast megalopolis from Maine through Virginia:
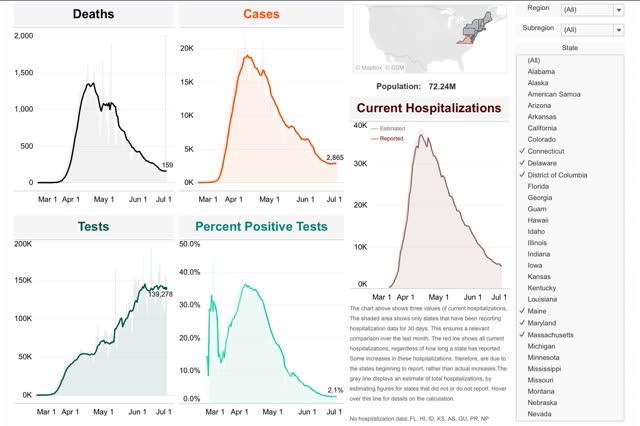
Cases have risen very slightly in the past few days, while hospitalizations have continued to fall which has increased the amount of free hospital beds to treat other illness. Deaths have flattened.
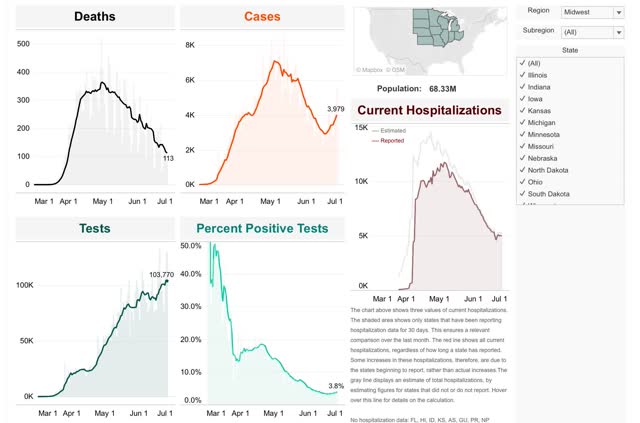
In the Midwest, cases have risen by about 25% in the past 12 days. Hospitalizations have flattened, while deaths have continued to decline:
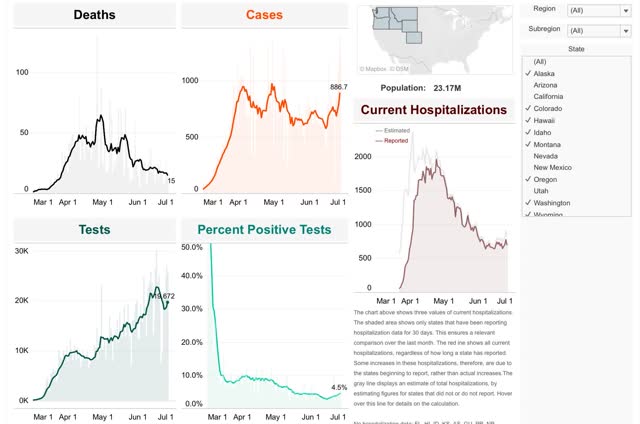
In the northern West, case started rising a month ago, after May 26. Hospitalizations bottomed two weeks later on June 7. Deaths started to creep up at the same time:
In the Southwest, cases never decreased. But there was an inflection point for increased cases on May 28, which had 3,528 new cases. By June 26, that had more than doubled to 8,758 new cases:
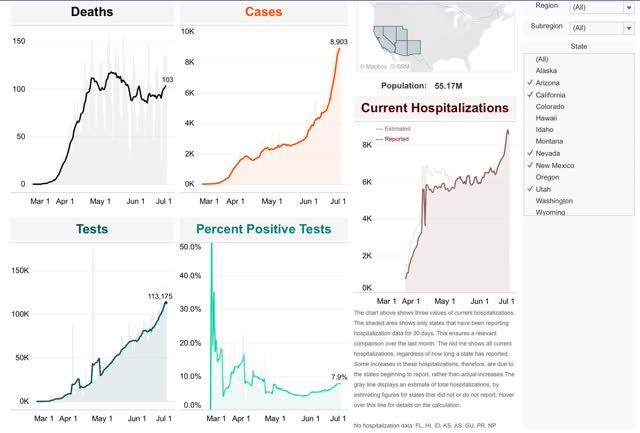
The inflection point in hospitalizations followed on June 14, since which time the number has increased by over 35%. The upward inflection in deaths followed on June 20.
Finally, in the Deep South, cases actually bottomed on April 27 at 4,337, with an upward inflection point at May 27, on which there were 5,171 new cases. Since then new cases have more than tripled to 17,748:
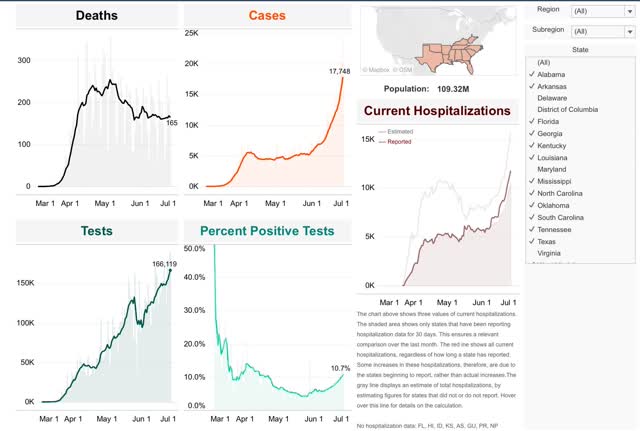
Hospitalizations reached their inflection point on June 6 at 5,791. Since then they have nearly doubled to 10,565. Deaths bottomed on June 18 at 160 and have risen slightly since then to 165.
In short, while there is considerable variation, in general deaths have lagged hospitalizations by about 1 to 2 weeks. We are now nearly 2 weeks after the bottom in hospitalizations for the US as a whole. Thus I expect deaths to start increasing, at least slowly, in the next few days.
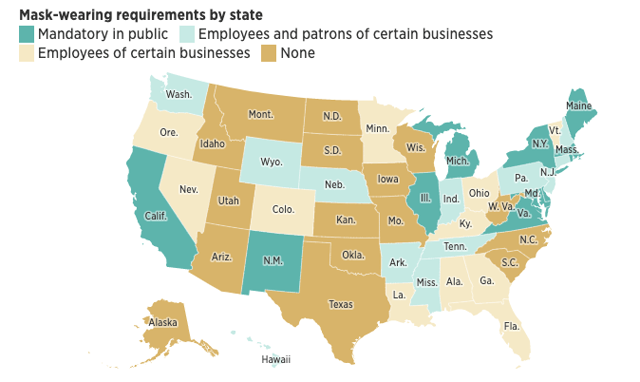
With the very notable exception of California on the one hand, and the sparsely populated States of the northern Plains and Rockies, mask-wearing, or the lack thereof, is highly correlated with increases or decreases in new cases.
Another big correlation with new cases has been restaurant reopening, as shown in the below graph comparing cases with restaurant spending:
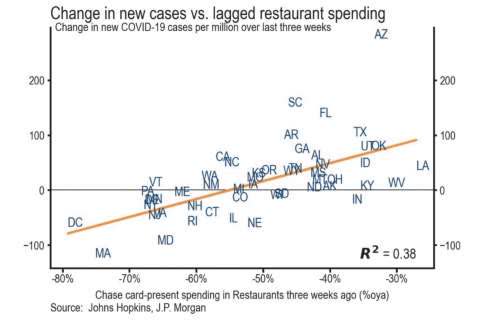
Confined indoor spaces, air-conditioned recirculating ventilation, and the necessary lack of mask-wearing in order to eat or drink sure seems to be a recipe for spreading the virus.
And if the public does not have confidence that the virus has been contained, the economy is not going to be able to sustain reopening for very long, as shown in the below graph of consumer confidence by region:
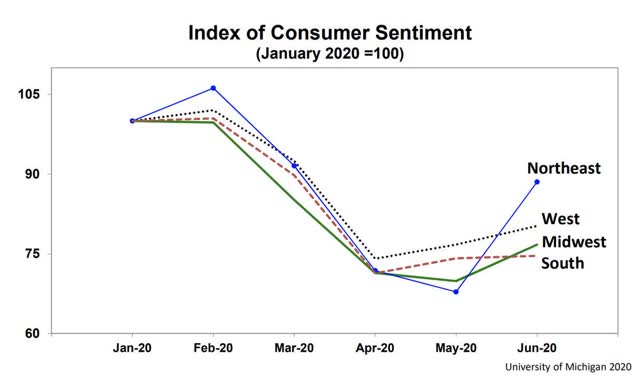
Only in the Northeast, where the virus has been very well contained (for now) has there been a big rebound in consumer confidence.
Finally, it’s worth noting that this is even showing up in the stock market:

As of Friday, the S&P 500 was less than 5% above where it was at its January 2018 peak. If deaths start to rise substantially, as I believe they will, portions of the economy are going to shut right back down again, whether by law or regulation, or simply because customers stop showing up.
After Asking Americans to Sacrifice in Shutdown, Leaders Failed to Control Virus
NY Times – Sabrina Tavernise, Frances Robles and Louis Keene – June 27
WASHINGTON — More than four months into fighting the coronavirus in the United States, the shared sacrifice of millions of Americans suspending their lives — with jobs lost, businesses shuttered, daily routines upended — has not been enough to beat back a virus whose staying power around the world is only still being grasped.
The number of new U.S. cases this last week surged dangerously high, to levels not ever seen in the course of the pandemic, especially in states that had rushed to reopen their economies. The result has been a realization for many Americans that however much they have yearned for a return to normalcy, their leaders have failed to control the coronavirus pandemic. And there is little clarity on what comes next.
“There has to be a clear coherent sustained communication, and that has absolutely not happened,” said Dr. William Schaffner, an infectious diseases specialist at Vanderbilt University in Nashville. “We’ve had just the opposite and now it’s hard to unring a whole series of bells.”
There was “real hubris” on the part of public health officials at the very start, Dr. Schaffner said, that the United States could lock down and contain the virus as China had. That futile hope helped create an unrealistic expectation that the shutdown, while intense, would not be for long, and that when it was lifted life would return to normal.
That expectation was reinforced by President Trump, who has downplayed the severity of the crisis, refused to wear a mask and began calling for states to open even as the virus was surging. A lack of federal leadership also meant that states lacked a unified approach.
With no clear message from the top, states went their own ways. A number of them failed to use the shutdown to fully prepare to reopen in a careful manner. As Americans bought precious time trying to keep the virus at bay, experts advised that states urgently needed to establish a robust system for tracking and containing any new cases — through testing, monitoring and contact tracing. Without this, the pandemic would simply come roaring back.
Testing and contact tracing efforts were ramped up, but not enough in some places. Even states that did embark on ambitious plans to do contact tracing struggled. Health officials in Massachusetts, which has one of the country’s most established tracing programs, said in May that only about 60 percent of infected patients were picking up the phone.
Just as the country needed to stay shut down longer, many states — mostly with Republican governors — took their foot off the brake, and Mr. Trump cheered them on.
In early May, when more than half of U.S. states had begun reopening parts of their economies, most failed to meet the nonbinding criteria recommended by the Trump administration itself to resume business and social activities.
The White House’s nonbinding guidelines suggested that states should have a “downward trajectory” of either documented coronavirus cases or of the percentage of positive tests.
Yet most states that were reopening failed to adhere to even these ill-defined recommendations. They had case counts that were trending upward, positive test results that were rising, or both, raising concerns among public health experts.
The virus has proved formidable around the world, resisting global efforts to find a treatment, refusing to fade in summer weather and unrelenting in exploiting weaknesses in government responses, even in countries whose responses to the virus have been considered a success — and where the threat seemed tamed.
Germany, whose handling of the virus was considered a success, had to reimpose lockdowns on two counties where there was a spike of cases in slaughterhouses and low-income housing blocks. Singapore experienced a second wave of infections in April.
And in China, which adopted some of the world’s strictest measures to contain the virus, Beijing suffered this month a new surge of cases, causing flights to be canceled and schools to be closed.
Much of the challenge stems from major gaps in knowledge about how the virus works. In addition to chasing a vaccine, scientists around the world are still trying to unravel important mysteries, including how long immunity lasts after infection and why some people get so much sicker than others.
For Americans, a troubling new reality set in this week: Even as some parts of the country, like New York, were finally getting the virus under control, it was surging anew in others, like a terrifying sequel, threatening lives and livelihoods.
New virus cases were on the rise in 29 states on Friday as the outlook worsened across much of the nation’s South and West.
On Saturday, Florida reported more than 9,500 new coronavirus cases, beating its record for the second consecutive day. At least 980 new cases were added in Nevada, more than double the state’s previous daily high. And in South Carolina, officials announced more than 1,600 new cases, nearly 300 more than the previous record, set a day before.
In Florida and Texas, governors closed bars on Friday, as they scrambled to control what appeared to be a brewing public health catastrophe. All this is leaving people with a strange sense of déjà vu and a bitterness at public officials for what felt like a fumbling of people’s sacrifices. …
Many Americans started in the pandemic with a strong feeling of solidarity, not unlike the days after Sept. 11th, 2001. They closed their businesses, stayed inside, made masks and wiped down their groceries. In a country often riven by politics, polls showed broad agreement that shutting down was the right thing to do.
But months of mixed messages have left many exhausted and wondering how much of what they did was worth it. …
The plight of California has served as a warning that even states that were more aggressive in their strategies have not been entirely successful.
California, which had the first stay-at-home order in the United States this spring, allowed businesses to reopen weeks ago as the state felt it had the virus under control. That seems to be changing: California reported its highest single-day total this week and announced more than 5,600 new cases on Friday.
The rise comes despite the fact that the state has hired and trained thousands of contact tracers. It has also dramatically ramped up testing. And the millions of face masks that were promised early on have begun to finally materialize. …
In recent weeks, some conservatives said they had an additional concern: After weeks of being told that going to church, attending funerals, and participating in protests was a willful, careless spurning of science, political leaders and some public health officials condoned — and even joined — the crowds protesting the killing of George Floyd. …
American’s trust in the federal government has been falling for decades, but the recent months of muddied messaging have left many even more skeptical of public officials. …
Dr. Schaffner offered a bleak prognosis for the country’s next chapter with the virus. He said he did not expect the country to return to a full lockdown, so in order to contain the infection people would have to begin to change behaviors in ways that were uncomfortable, unfamiliar — wearing masks, not gathering in large groups indoors, staying six feet apart.
“The only alternative until we have a vaccine is all of these behavioral interventions that we know work,” he said. But, he added, “The governors are all on different pages. It is no wonder that the average person is confused.” …
https://covidtracking.com/blog/why-changing-covid-19-demographics-in-the-us-make-death-trends-harder-to
…
What we only sort of know: the changing demographics of the disease
Some anecdotal and statistical evidence suggests that the average age of people with COVID-19 is declining, which complicates expectations that deaths will increase in step with new cases. On June 16, for instance, Texas Gov. Greg Abbott said that a majority of people testing positive in three counties were under 30, which he said “typically results from people going to bars”; Dr. David Persse, public health authority of the Houston Health Department, told The Texas Tribune that “it is my current theory that elder persons have become more vigilant in taking precaution.” Florida Gov. Ron DeSantis has also said that infections are starting to skew younger.
In the Dallas-Fort Worth region of Abbott’s state, the University of Texas Southwestern reports that the age distribution of positive COVID-19 tests has shifted dramatically from March to June, with a peak under 30 years old. Hospitalizations and ICU admissions in the DFW region have also shifted younger if less dramatically; 50% of hospitalized patients are under 50, as are 30% of ICU patients.
In California in mid-May, three-quarters of all COVID-19 cases were split evenly between residents 18-34, 35-49, and 50-64, at almost exactly 25% for each group. By June 13, the 18-34 group represented a third of cases, while those 50-64 fell to 19%. Over a similar timeframe in Florida, the median age of people testing positive for COVID-19 fell from 54 to 35.
Untangling this shift in age groups from increased testing is a challenge. With additional testing available, more people in lower-risk populations are likely being tested now than when tests were being strictly rationed to severe cases. As businesses reopen across the country, workplace testing may also increase case numbers for the working-age population, and perhaps particularly younger-skewing service workers. Testing, however, is not universally adequate; local and regional spikes in cases are putting pressure on testing infrastructure. The Upshot reports that the testing capacity situation is “acute” in Arizona. In Florida, The COVID Tracking Project’s data indicates testing has actually slowed by 10% in the last two weeks.
In a Twitter thread, University of Florida biostatistics professor Dr. Natalie Dean offers three possible explanations for why the median age of cases might be falling, and what data signals we should look for.
If it’s simply a matter of more testing, hospitalizations should not increase, and test positivity should decline or hold steady. In the South and West, positivity rates appear to be rising, but regional numbers can mask very different state trends. In Texas, Florida, and Arizona, test positivity and cases are both rising; in California, by contrast, new cases are way up but the positivity rate has remained at five percent in June, and in Georgia the positivity rate is up just two percentage points while testing is up.
If “elderly people are more cautious,” then cases, test positivity, and hospitalizations should decline. In the Northeast, tests are way up, positivity is way down, and new cases are flat. In New Jersey, new daily cases are down to 10% of April peaks, and hospitalizations have dropped precipitously. New daily cases in Connecticut have been in the double digits for the past couple weeks, and hospitalizations are down to 124 as of June 23 from over a thousand in mid-May.
If younger people are less cautious—or if they’re more exposed as young service workers return to their jobs—cases, test positivity, and hospitalizations should rise. This is happening in Texas and Arizona. Cases and test positivity are up in Florida; statewide hospital data was only available for a few days in May before the state removed it from public view, but in Miami-Dade County, hospitalizations increased from 601 to 776 from June 9 to June 22.
Dean ultimately concludes that it’s slightly too early to tell, but the real answer is likely a combination of all three, and that better age-stratified data is needed. High-quality samples exist for the country as a whole, but as we’ve seen, trends vary greatly from state to state and even city to city. The United States is a big country that needs a lot of detailed data.
The best source for nationwide data on testing and positivity by age is the CDC’s COVID-NET, a hospital surveillance network that serves as a sample—the data is very detailed, but it’s from only 250 hospitals spread across 14 states. COVID-NET data is best summarized in the CDC’s weekly COVIDView reports. Looking at that data, Dr. Trevor Bedford of the Fred Hutchinson Cancer Research Center finds hints of Dean’s explanations: a substantial decline in positivity among tests in the 50-plus age group from early April to early June, and a slower decline among younger age groups, with signs of a plateau. He also found a very small increase in cases in the below-50 age group in that same time. (Disclosure: Both Dean and Bedford are members of The COVID Tracking Project’s advisory board.)
What changing age demographics have to do with deaths
In areas where younger adults are driving new infections, we might not see deaths spike until infections overflow into more vulnerable populations. “If what is happening are outbreaks in young people, it seems likely that these young people will go on to transmit to others in their communities,” Dean writes in an email. “This spillover would cause a subsequent rise in cases among older people, followed by a lagged rise in deaths.” She points to a pattern in Florida in which new cases in the 0-44 age group began climbing gradually in early-mid May, echoed by a smaller climb in the 45+ age group in late May-early June. Cases in the first age group began increasing rapidly around the beginning of June, a worrisome portent for the more vulnerable 45+ age group.
…
June 28, 2020
Coronavirus
US
Cases ( 2,621,662)
Deaths ( 128,315)
India
Cases ( 549,196)
Deaths ( 16,487)
UK
Cases ( 311,151)
Deaths ( 43,550)
Mexico
Cases ( 212,802)
Deaths ( 26,381)
China
Cases ( 83,500)
Deaths ( 4,634)
June 28, 2020
Coronavirus
US
Cases ( 2,629,436)
Deaths ( 128,391)
https://twitter.com/paulkrugman/status/1277375824187047936
Paul Krugman @paulkrugman
Based on positivity rates, Houston looks as if it’s only around a week behind AZ. Florida not much more. And they *still* are barely reversing their reopening 1/
The COVID Tracking Project @COVID19Tracking
Every day, the data from Arizona looks worse. Deaths are now moving upward. The 7-day average for deaths reported by the state has now crossed 100.Show this thread
6:58 PM · Jun 28, 2020
I haven’t seen people make this point as clearly as it should be made: Trump and his allies have committed the same deadly sin three times. First, they refused to face up to the threat; then they pushed for a premature end to lockdown; now they’re dithering as Covid-19 surges 2/
Each time they were looking for political gain — let’s not worry the stock market; let’s tell a story about recovery in time for the election; let’s not admit that we were wrong a month ago. So they gambled with tens of thousands of American lives. And the nation lost 3/
So let’s be clear: these weren’t honest errors made in good faith. Trump, but also people like DeSantis and Hannity, played cynical games with American lives, and bear responsibility for many thousands of unnecessary deaths. 4/
The COVID Tracking Project @COVID19Tracking
Florida’s refusal to report current COVID-19 hospitalization numbers leaves us without a critical data point for one of the worst outbreaks of the summer surge.
https://www.nytimes.com/2020/06/28/health/coronavirus-delirium-hallucinations.html
June 28, 2020
‘They Want to Kill Me’: Many Covid Patients Have Terrifying Delirium
Paranoid hallucinations plague many coronavirus patients in I.C.U.s, an experience that can slow recovery and increase risk of depression and cognitive issues.
By Pam Belluck
June 28, 2020
Coronavirus
US
Cases ( 2,636,550)
Deaths ( 128,436)
https://news.cgtn.com/news/2020-06-29/Cholesterol-lowering-drugs-help-reduce-COVID-19-deaths-study-RHXVbCLmP6/index.html
June 29, 2020
Cholesterol-lowering drugs help reduce COVID-19 deaths: study
Commonly used cholesterol-lowering statin drugs may help reduce the death rate in hospitalized COVID-19 patients, according to a new study * published in the journal Cell Metabolism….
* https://www.cell.com/cell-metabolism/pdfExtended/S1550-4131(20)30238-2
Correcting reference article link:
https://news.cgtn.com/news/2020-06-29/Cholesterol-lowering-drugs-help-reduce-COVID-19-deaths-study-RHXVbCLmP6/index.html
June 29, 2020
Cholesterol-lowering drugs help reduce COVID-19 deaths: study
Commonly used cholesterol-lowering statin drugs may help reduce the death rate in hospitalized COVID-19 patients, according to a new study * published in the journal Cell Metabolism….
* https://www.cell.com/cell-metabolism/fulltext/S1550-4131(20)30316-8
Half a million people are dead as confirmed virus cases top 10 million
The global total of deaths from the coronavirus has passed 500,000, according to a New York Times database, while the number of confirmed cases surpassed 10 million.
The grim markers were hit on Sunday as countries around the world struggled to keep new infections from reaching runaway levels while simultaneously trying to emerge from painful lockdowns.
In April, roughly a month after the World Health Organization declared the outbreak a pandemic, deaths topped 100,000. In early May, the figure climbed to 250,000.
More than a quarter of all known deaths have been in the United States.
The number of confirmed infections — which took about 40 days to double — may be substantially underestimated, public health officials say. Data released last week by the Centers for Disease Control and Prevention indicated that the actual figures in many regions are probably 10 times as high as reported.
The Times has also found that the actual death toll in the United States and more than two dozen other countries is higher than has been officially reported. Limited testing availability has often made it difficult to confirm that the virus was the cause of death. …
Gilead prices coronavirus drug at $2,340 for rich countries
via @BostonGlobe
The maker of a drug shown to shorten recovery time for severely ill COVID-19 patients says it will charge $2,340 for a typical treatment course for people covered by government health programs in the United States and other developed countries.
Gilead Sciences announced the price Monday for remdesivir, and said the price would be $3,120 for patients with private insurance. The amount that patients pay out of pocket depends on insurance, income and other factors.
“We’re in uncharted territory with pricing a new medicine, a novel medicine, in a pandemic,” Gilead’s chief executive, Dan O’Day, told The Associated Press.
“We believe that we had to really deviate from the normal circumstances” and price the drug to ensure wide access rather than based solely on value to patients, he said.
The 250,000 treatment courses that the company had donated to the U.S. and other countries will run out in about a week, and the prices will apply to the drug after that. …
It is a 10 dose treatment.
June 29, 2020
Coronavirus
US
Cases ( 2,650,771)
Deaths ( 128,518)
India
Cases ( 559,910)
Deaths ( 16,757)
UK
Cases ( 311,965)
Deaths ( 43,575)
Mexico
Cases ( 216,852)
Deaths ( 26,648)
China
Cases ( 83,512)
Deaths ( 4,634)
“We believe that we had to really deviate from the normal circumstances” and price the drug to ensure wide access rather than based solely on value to patients, Dan O’Day said.
[ This is a critically important passage. About a decade ago, drug companies began to price drugs not on costs of production but on the value of a drug to patients. A sort of Clint Eastwood, “Do you feel lucky today? pricing. Genentech, controlled by Roche, began this pricing. ]
http://www.nytimes.com/2006/02/15/business/15drug.html
February 15, 2006
A Cancer Drug Shows Promise, at a Price That Many Can’t Pay
By ALEX BERENSON
Doctors are excited about the prospect of Avastin, a drug already widely used for colon cancer, as a crucial new treatment for breast and lung cancer, too. But doctors are cringing at the price the maker, Genentech, plans to charge for it: about $100,000 a year.
That price, about double the current level as a colon cancer treatment, would raise Avastin to an annual cost typically found only for medicines used to treat rare diseases that affect small numbers of patients. But Avastin, already a billion-dollar drug, has a potential patient pool of hundreds of thousands of people — which is why analysts predict its United States sales could grow nearly sevenfold to $7 billion by 2009.
Doctors, though, warn that some cancer patients are already being priced out of the Avastin market. Even some patients with insurance are thinking hard before agreeing to treatment, doctors say, because out-of-pocket co-payments for the drug could easily run $10,000 to $20,000 a year.
Until now, drug makers have typically defended high prices by noting the cost of developing new medicines. But executives at Genentech and its majority owner, Roche, are now using a separate argument — citing the inherent value of life-sustaining therapies.
If society wants the benefits, they say, it must be ready to spend more for treatments like Avastin and another of the company’s cancer drugs, Herceptin, which sells for $40,000 a year….
[ Clint Eastwood style drug pricing, beginning in about 2006. “Do you feel lucky today?” ]
Until now, drug makers have typically defended high prices by noting the cost of developing new medicines. But executives at Genentech and its majority owner, Roche, are now using a separate argument — citing the inherent value of life-sustaining therapies.
If society wants the benefits, they say, it must be ready to spend more for treatments like Avastin and another of the company’s cancer drugs, Herceptin, which sells for $40,000 a year….
[ This is both having a patent monopoly but being in a position to charge a patient for the value of life. This is an inherently immoral pricing policy, but largely taken to be reasonable. I pointed this out about the pricing of water in Bolivia, so that poorer Bolivians could not afford water, a policy defended from the New York Times to a prominent University of California neoliberal economist. ]
anne:
I get the feeling, you have not seen much of my commentary. Can You Patent the Sun? The story on Herceptin is in that post also.
About Sweden, where the government chose to more or less let the coronavirus run through the country, along with having a remarkably high ratio of deaths to confirmed coronavirus cases, 8.1%, Swedish data have recently been withheld from the public. This while the Swedish official who designed the do not interfere policy criticizes approaches to limit the infection spread taken in other countries.
I get the feeling, you have not seen much of my commentary….
[ Sorry, I have read no commentary on this blog before mere days ago. However, I find your writing excellent and am grateful. ]
anne:
Don’t butter me up too much. It may go to my head and I will be asking Dan for a raise.
The one post I iinked to uses a Swiss source SwissInfo as one of its sources and Swiss public TV to report on the Swiss company Roche, Herceptin and Mabthera.
I spent a lot of time on this one. Much of this research has gone by the wayside due to the pandemic.
A while ago, there were articles * about the Indian experience in the state of Kerala with the coronavirus. Kerala had managed the outbreak really well, while I wondered about a range of managing in other Indian states. I have no idea what is occurring in Kerala now and will try to find out, but there seems to be a fearsome number of new cases in India just now.
What has happened?
* https://www.project-syndicate.org/commentary/kerala-model-for-beating-covid-19-by-shashi-tharoor-2020-05
May 11, 2020
The Kerala Model
June 29, 2020
Coronavirus
US
Cases ( 2,656,061)
Deaths ( 128,574)
India
Cases ( 567,536)
Deaths ( 16,904)
https://www.nytimes.com/2020/06/29/upshot/coronavirus-tests-unpredictable-prices.html
June 29, 2020
Two Friends in Texas Were Tested for Coronavirus. One Bill Was $199. The Other? $6,408.
It’s an example of the unpredictable way health prices can vary for patients who receive identical care.
By Sarah Kliff
anne:
Surprise billing, out-of-network, or not on list of approved treatments.
https://www.nytimes.com/2020/06/28/us/coronavirus-hospital-houston.html
June 28, 2020
‘Feeling Like Death’: Inside a Houston Hospital Bracing for a Virus Peak
As young patients fill new virus wards, Houston Methodist is calling nurses to work extra shifts and ramping up its testing efforts.
By Sheri Fink
[ Notice the word “young,” but “older” should be as fearsome for all of us. ]
Hey:
If you can access this clip, it is some pretty scary stuff. They pull a ventilator out of a guy’s (?) mouth and it is all gunky from his lungs. A clip of a nurse who caught Covid from pumping on a person’s chest and the person breaths into his face. She is talking to her two young daughters in the clip . . . almost in tears. They should show this nationally and scare the crap out of the mask less dummies. This is on CNN. Google it: “‘Feeling Like Death’: Inside a Houston Hospital Bracing for a Virus Peak.”
June 29, 2020
Coronavirus
US
Cases ( 2,671,605)
Deaths ( 128,721)
Still about 5% or 1 in 20 die once they contract Covid. I expect the death rate to increase since Texas, Florida, Arizona, California, etc. do not give a damn about people and are hell-bent on protecting business.
A month ago, who had ever heard of ‘herd immunity’? It would
be better if the anti-vaxers took one for the team, but if that’s
not to be, lets just get that oh-so-imminent vaccine out to
those who want it.
Fauci warns US “unlikely” to reach herd immunity if too many refuse vaccine
via @CBSPolitics
Washington — Dr. Anthony Fauci, one of the nation’s leading experts on infectious diseases, warned Sunday that it’s “unlikely” the U.S. will achieve herd immunity to the coronavirus if a portion of the population refuses to get a coronavirus vaccine.
In an interview that aired Sunday as part of the Aspen Ideas Festival, Fauci said he would “settle” for a coronavirus vaccine that is between 70% and 75% effective, “because that would bring you to that level that would be herd immunity level.”
But when asked by CNN senior medical correspondent Elizabeth Cohen whether the U.S. can get to herd immunity if 25% of the population refuses to get a coronavirus vaccine with that rate of effectiveness, Fauci said, “No, unlikely.” …
As for vaccines, we should all be taking the flu vaccine shot when that is ready this summer. Also, remember that Angela Merkel was given a pneumonia vaccination a couple of months ago so look to that as well. These shots are covered by any insurance.
https://www.nytimes.com/2020/06/29/opinion/obamacare-coronavirus-republicans.html
June 29, 2020
Obamacare Versus the G.O.P. Zombies
Ten years of failed promises to come up with something better.
By Paul Krugman
Covid-19 cases are surging in states that took Donald Trump’s advice and reopened for business too soon. This new surge — is it OK now to call it a second wave? — is, on average, hitting people younger than the initial surge in the Northeast did. Perhaps as a result, rising infections haven’t been reflected in a comparable rise in deaths, although that may be only a matter of time.
There is, however, growing evidence that even those who survive Covid-19 can suffer long-term adverse effects: scarred lungs, damaged hearts and perhaps neurological disorders.
And if the Trump administration gets its way, there may be another source of long-term damage: permanent inability to get health insurance….
http://www.xinhuanet.com/english/2020-06/30/c_139176258.htm
June 30, 2020
Nearly half of new COVID-19 cases in U.S. Louisiana among people under 30
June 29, 2020
Coronavirus
US
Cases ( 2,680,636)
Deaths ( 128,771)
Yes, yes, I know who the president is and I know how unfortunate we are, however, the extent of the devastation done by the coronavirus needs to be considered a general political failure. Such an institutional or human rights failure needs careful consideration and I am afraid just blaming the president is not enough or will teach us too little.
Hi Anne
http://angrybearblog.com/2020/06/what-will-history-say.html#comments
The 2020 Pandemic: The US Government was incapable of leading the efforts to limit the ravages of the Pandemic. The US Government’s response was a failure in almost every way. There was inadequate preparedness; funding to those agencies charged with meeting the challenge had been cut as part of spending reduction measures. The $billions saved wound up costing $trillions. Political considerations were given precedence over the facts, over science. The US Government was incapable of performing the functions of Government.
A cohesive commentary. I still owe you an answer on drugs and how the epidemic evolved from the eighties.
Hi Ken, and excuse me for not commenting earlier that you are writing splendidly. I read your earlier essay, then was distracted, so I am sorry for not being grateful and encouraging,
Here, I agree but we need several narrow questions to answer as to why we were incapable. I am thinking, so you think too.
Look to the way in which a community infection was discovered and evidently controlled in Beijing in mere days.
Open the graph:
https://news.cgtn.com/news/2020-06-30/Beijing-reports-7-new-COVID-19-cases-all-locally-transmitted-RJHAcE3VwQ/index.html
June 30, 2020
Beijing reports 7 new COVID-19 cases, all locally transmitted
The Beijing Health Commission said on Tuesday that 7 new locally transmitted COVID-19 cases were recorded on Monday, raising total infections to 324 since June 11, when the first case from Beijing’s Xinfadi market cluster was detected.
The 7 cases were reported in 2 districts in Beijing: 6 in Fengtai, 1 in Daxing.
Beijing also registered 1 asymptomatic case on Monday, the health authority said.
[ https://pbs.twimg.com/media/EbuJv3MU4AA0Wu0?format=jpg&name=4096×4096 ]
https://news.cgtn.com/news/2020-06-30/Chinese-mainland-reports-19-new-COVID-19-cases-7-in-Beijing-RJFqVbXekU/index.html
June 30, 2020
Chinese mainland reports 19 new COVID-19 cases, no new deaths
A total of 19 new COVID-19 cases were reported on the Chinese mainland on Monday, of which 8 were local transmissions and 11 were from overseas, with no additional deaths, according to Chinese health authorities on Tuesday.
Seven of the locally transmitted cases were registered in Beijing, the other in Shanghai, the National Health Commission said in its daily report.
The total number of confirmed cases on the Chinese mainland stands at 83,531 and the cumulative death toll at 4,634, with 99 asymptomatic patients under medical observation.
The total confirmed cases in the Hong Kong and Macao special administrative regions and the Taiwan region are as follows:
Hong Kong: 1,203 (1,105 recoveries, 7 deaths)
Macao: 46 (45 recoveries)
Taiwan: 447 (435 recoveries, 7 deaths)
Chinese mainland new locally transmitted cases
https://news.cgtn.com/news/2020-06-30/Chinese-mainland-reports-19-new-COVID-19-cases-7-in-Beijing-RJFqVbXekU/img/8fec72663d6241429b460e3469bcf2ca/8fec72663d6241429b460e3469bcf2ca.jpeg
Chinese mainland new imported cases
https://news.cgtn.com/news/2020-06-30/Chinese-mainland-reports-19-new-COVID-19-cases-7-in-Beijing-RJFqVbXekU/img/39551b6ef58d4b5f873e517ae5da70b8/39551b6ef58d4b5f873e517ae5da70b8.jpeg
Chinese mainland new asymptomatic cases
https://news.cgtn.com/news/2020-06-30/Chinese-mainland-reports-19-new-COVID-19-cases-7-in-Beijing-RJFqVbXekU/img/78e651234c2648df8f253c31be88d5ca/78e651234c2648df8f253c31be88d5ca.jpeg
Monitor for cases continually and when a case whether community or imported is found:
Test, trace contacts, test and isolate; but do the work in earnest.
Masks must be worn; temperature checks must be conducted.
Protective gear for all medics.