COVID-19 progress, take 2
In response to the comment on my last post . . . rolling 7 day average death rates with the peak for each country set to 100.
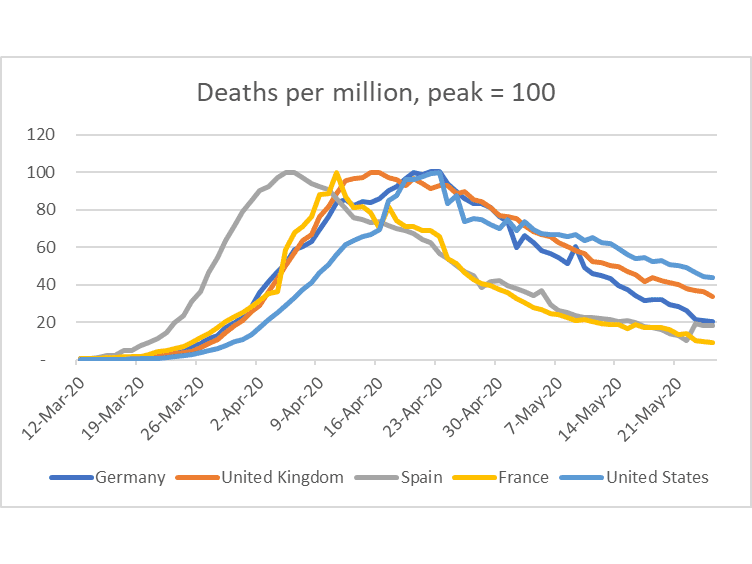 We peaked later than most countries other than Germany, which seems to be making better progress than us. We may be doing as well (or as badly) as the U.K. It seems like France and Spain are also outperforming the U.S. on this metric.
We peaked later than most countries other than Germany, which seems to be making better progress than us. We may be doing as well (or as badly) as the U.K. It seems like France and Spain are also outperforming the U.S. on this metric.
Normalizing peak to 100 might not be a sensible way to present the data. I recall that the graphics of “flattening the curve“ was shallower on both the way up and down. Maybe those are just pictures but maybe a higher peak must have a faster decrease if the pool of those most likely to succumb is fairly fixed.
This is a very interesting virus. IMHO curves by the country does not tell us much as local conditions drastically differ within each single country. Like is ‘Lies, damned lies, and statistics” 😉
As death rates in many countries include both from COVID-19 and “with COVID-19” those curves can even be misleading. Only excessive deaths rom previous years average make some sense in country to country comparison.
First of all, the spread is highly concentrated in large multi-million cities. For example, NYC metropolitan area accounts for ~40% of attributed to COVID-19 deaths and essentially dominate the country stats.
But the situation in NYC and Hudson river area of NJ is not all the USA. Outside large cities and their immediate suburbs the USA is affected much less.
For example, in many towns 70 miles west from NYC nobody knows even one person who became infected.
The second interesting feature of this virus is that it mainly kills old (and, especially, very old) as well as obese (“diabetic” in the USA is, in a way, a code name for the morbidly obese), and hypertonics. Those three categories cover around 80% of all deaths, Add to them people with other serious medical conditions and you probably get 90%.
As such hey reflect as much the level of inequality and “aging population” phenomena, as the government reaction..
If so, the question arise whether the sacrifices forced by prolonged quarantine are justified by the severity of the epidemic (the first month was probably justifiable as it was unclear what kind of danger we face) ?
Also Fauci fake prognoses (based on now discredited Ferguson models) now became serious liability both for him and for Trump (Fauci probably is a goner; hopefully Trump is too )
And while Trump administration as a whole demonstrated amazing incompetence in the process, states amplifies it with arbitrary measures of their own and idiotic moves. Remember Cuomo stupid (and expensive) quest for more ventilators, for more hospital beds, and his controversial directive ordering nursing homes to admit COVID-19 patients..
I also doubt that opening shops in the areas with zipcodes that registered zero or single digit of cases can change something. Just look how unequal the NY counties are:
https://www.worldometers.info/coronavirus/usa/new-york/
For example, I doubt that there is much value in continuation of quarantine in the bottom dozen of counties in this table.
There is no surprise that in many western counties the NY and NJ governors are now viewed as enemies of people and effigies were burned on Memorial day 😉
At the same time the problems for NYC and vicinities are not gone. They now look even more serious. Homeless, subways, packed buses and elevators are pretty efficient means of spreading the virus and will remains so. Population density is also a huge, insurmountable factor.
So here one size definitely does not fit all and the work should be done differently in individual areas.
In may areas closing shops and restaurants was probably redundant and closing of entertainment (especially night clubs and cinemas) and churches (which are mostly attended by old people) as well as special protection measured for nursing homes and prisons might be sufficient.
Why is it very interesting?
Maybe because it is the first virus programmed with a priority to attack those who are greater than 65? It is an equal opportunity virus and anyone can catch it. If any person has secondary health issues, they have a great propensity to die, age aside. Older people have greater health issues more so than younger people.
It is called a pandemic and allowing people to wander around willy-nilly from place to place, socialize at close quarters, and not take adequate precaution to control the spittle coming from their mouth spreads the virus of which little was know about in the beginning and ignored for two months. There is Sweden practicing herd immunity who has had ~7% of its population infected and the US with ~2% of its population infected. A minority of the population in Michigan is playing a game of which they toss aside the rules of engaged safety in society for a few moments of freedom. Ten days later Michigan sees a spike in deaths and new cases, one in ten die. The rural areas are being infected because of the travel of those who believe their liberty is more important than the liberty of others who they have purposely infected.
The nation was inhibited by a stupid president and a Republican party who has no interest in the population. The virus should have been called out no later than February 1st and Fauci knew of the issues sooner.
https://www.nytimes.com/2020/05/25/world/europe/coronavirus-uk-nursing-homes.html
May 25, 2020
On a Scottish Isle, Nursing Home Deaths Expose a Covid-19 Scandal
At the Home Farm nursing home on the Isle of Skye, more than a quarter of its residents died and nearly all were infected with coronavirus. Families are furious.
By Benjamin Mueller
On the Isle of Skye off the western coast of Scotland, residents thought they had sealed themselves off from the coronavirus. They shuttered hotels. Officials warned of police checks. Traffic emptied on the only bridge from the mainland.
But the frailest spot on the island remained catastrophically exposed: Home Farm, a 40-bed nursing home for people with dementia. Owned by a private equity firm, Home Farm has become a grim monument of the push to maximize profits at Britain’s largest nursing home chains, and of the government’s failure to protect its most vulnerable citizens.
Today, all but seven of the residents have been stricken. More than a quarter are dead.
The virus has ravaged nursing homes across Europe and the United States. But the death toll in British homes — 14,000, official figures say, with thousands more dying as an indirect result of the virus — is becoming a defining scandal of the pandemic for Prime Minister Boris Johnson.
By focusing at first on protecting the health system, Mr. Johnson’s strategy meant that some infected patients were unwittingly moved from hospitals and into nursing homes. Residents and staff members were denied tests, while nursing home workers begged in vain for protective gear….
[ “Mr. Johnson’s strategy meant that some infected patients were unwittingly moved from hospitals and into nursing homes.”
There could be no “unwitting” movement of infected patients from hospitals and into nursing homes, when the Chinese had in January shown the critical importance of isolating infected patients. ]
Likbez,
Your commentary is indeed rather peculilar. You somehow suggest the normalized curves shown do not tell us much because of the supposed vast differences between nations. How does that affect this specifically? What we see is that the US has a slower decline in cases than these other nations. I see nothing in your comments that follow that provide any useful explanation of this.
Indeed, you seem to seriously miss the point. In all these nations the most cases happened in densely populated urban areas. Those cases are now getting under control in most of those nations in the largest metro areas, including certainly the New York metro area. I also think there is basically nobody opposed to having within-state different approaches to reopening, and we are seeing that in many states, including Virginia and New York. Exactly why are people in western New York burning Cuomo in effigy, which you seem to approve of?
As it is, you simply miss that probablyi the major reason US is having its clases decline mroe slowly is that we are having major new outbreaks happening. Were are thiese? Oh, lots of them are in these rural areas you think are so bloody safe. Granted, a lot of those have the special problem of having meat production facilities in them, but these other nations also have meat production facilities scattered around them. Why is US having a bigger problem than these others with this.
For the great length of your pretty pompous post, you pretty much missed the mark on a lot of pretty important points.
I’m trying to figure out what these curves tell us.
The curve for France seems to have the quickest rise and fall while the US curve has the slowest. Is this an artifact of a small, quickly handled pandemic as in South Korea or Taiwan? Is it because France had a particularly virulent epidemic, perhaps encouraged by COVID-19 parties, that burned out quickly?
What does this look like if you align the peaks?
My point is the form of the curve in the USA was partially distorted by the NY metropolitan areas with its huge and very specific problems and demographics. This area accounts for around 40% of cases.
Death per million normalize the number of death for the population of the whole county and that’s it.
But my pint is that the USA is not homogeneous country and will never be.
In this sense any “nationwide” statistics for the virus without exclusion of the NY metropolitan area for the USA is big fat lie. At least it is clear that it distorts the picture for the rest of the country.
We have core inflation which exclude food and energy, why we can’t have death without NY metropolitan area?
Another important point that the number of death as a statistics is another one big and fat lie. Or at least is very suspect. I would like to stress that only the difference between number of death for the particular period and average for several previous years has scientific value. Not the absolute number.
And what is interesting that for March 2020 COVID-19 epidemic was a lives saver. Such an interesting paradox.
There are essentially two outcomes of COVID-19 — one in this pneumonia does not develop, and the second in which virus pneumonia develops.
The only way to die from the virus is to die from virus pneumonia or complications (including organs failures due to the lack of oxygen).
Everything else (including gunshot wounds 😉 belongs to “with COVID-19” category and in the USA constitutes probably 80% of reported COVID-19 deaths. In other words, most of deaths reported are very sick people with significant percentage already of the death bed.
For people at the end of their life scan coronavirus is often the last straw that break the camel back, so to speak. Cutting this lifespan for several months or a couple of years at best.
And there is nothing special for this role of coronavirus. Flu acts exactly the same way: pneumonia as a flu complication is one of the most common ways for the old sick people to meet the creator.
Unfortunately we know very little about conditions in which pneumonia develops (there are probably some generic markers in play as well as sex and a couple of other metrics ) other that the main victims are obese (often morbidly obese), diabetics (which in the USA is almost synonym with obesity) and hypertonics (those are intersecting categories).
Chances for everybody else to get this (very dangerous indeed) virus pneumonia are approx. 100-1000 times less.