Coronavirus dashboard for April 2: nationwide lockdown nearly complete, but the surge in testing has completely stalled
Coronavirus dashboard for April 2: nationwide lockdown nearly complete, but the surge in testing has completely stalled
Here is the update through yesterday (April 1)
Close to 90% of the US population is now under lockdown, and it appears to be lowering the rate of exponential growth of new infections.
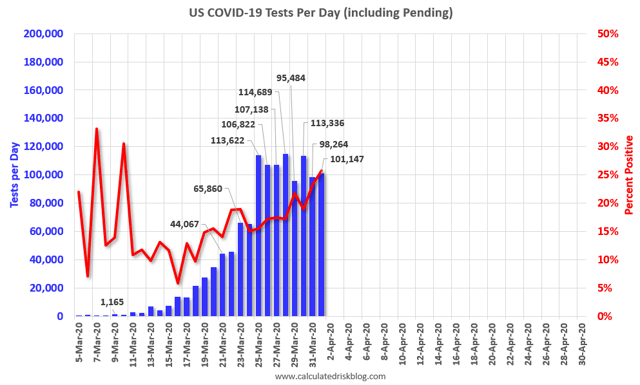
But testing in the past 6 days has plateaued at about 100,000/day and is not keeping pace at all with the growth in new infections. We will not be able to transition from the Sledgehammer of lockdowns to the scalpel of aggressive testing and quarantines until this changes. Deaths continue to climb at a steady exponential rate consistent with infections 2 weeks ago.
To transition to a South Korea style program, we also need to be able to trace infections and quarantine those newly infected. For that we need millions of thermometers, masks, and other equipment. There is no indication at all that this is happening.
The four most important metrics are starred (***) below.
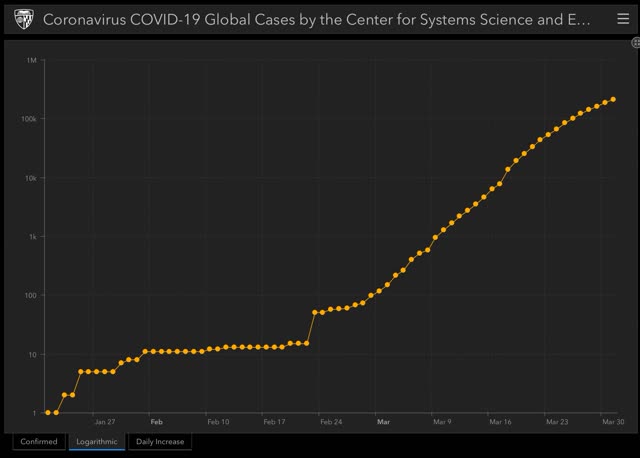
Number and rate of increase of Reported Infections (from Johns Hopkins via arcgis.com)
- Number: up +27,089 to 216,722 (vs. +25,023 on March 31)
- ***Rate of increase: day/day: 14% (vs. 34.6% baseline, 18% for the past week, and 15% on March 31)
The exponential rate of growth in US cases has begun to slow:
Ben Engebreth is started tracking coronvirus infection and testing numbers for each state, with graphs, here.
Number of deaths and infections and rate of increase of testing (from COVID Tracking Project)
- ***Number of deaths: Total 4700, up +954 day/day
- Rate: increase of 25% day/day vs. average of 26% in past week
- Number of tests: 100,989 down -3,128 vs. 104,117 on March 31 day/day
- Rate: decrease of -3.0% vs. number of tests previous day
Comparison of rates of increase in documented infections vs. testing
- Infections +14% vs. Tests -3% day/day
- Number: 100,989 new tests vs. 26,000 new diagnosed infections
- ***Ratio: 3.9:1
In South Korea, where aggressive testing has led to a near-total disappearance of new cases, the inflection point where the number of new daily cases plateaued was reached when the ratio of tests to new cases found reached 15:1. Any ratio less than that suggests that not enough testing is being done. Yesterday’s ratio of 3.9:1 continues to show that testing is falling further and further behind the level of new infections:
US States (+DC and PR) and population in total lockdown, business lockdown, and partial restrictions
- ***Total lockdown: 37 States (FL, GA, MS, OK^^ joined in last 24 hours), 268.0 million, 80.8%
- ***Business lockdown: 6 States (KY, MA, NV, PA*, SC*, TN*) 39.2 million, 11.8%
- Partial restrictions on business (bars, restaurants): 6 States (AL, IA, MO*, ND, UT*, WY) 18.8 million, 5.7%
- School closure only: 2 States (AR, SD) 3.9 million, 1.2%
- No mandatory restrictions: 1 State (NE) 1.9 million, 0.6%
Following Trump’s reversal on Easter Sunday openings, almost all of the holdout States in Dixie have implemented lockdowns. Nearly 90% of the US population is now under stay at home orders:
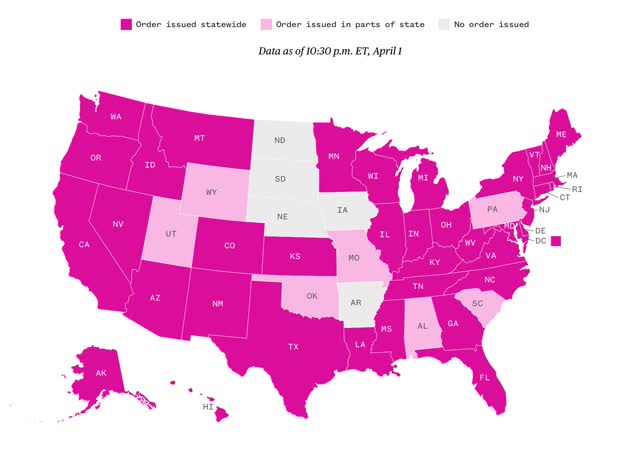
- Almost 90% of the total US population is under total lockdown.
- “Social distancing” and lockdowns appear to have lowered the growth rate of new infections.
- But travelers from States that resisted lockdowns will re-seed new outbreaks in those that went to lockdowns early
- The number of daily tests has stalled at about 100,000. So long as the virus keeps spreading at an exponential rate, even a lower one, we are falling further and further behind, I.e., we are failing to catch more new infections. The longer this continues, the longer it will be until total lockdowns can be lifted – because we don’t have the wherewithal to go to a “South Korea” style regimen of pervasive testing and quarantines.
- Since the Trump Administration will continue to fail, it is up to the States to band together to order emergency production of masks, tests, thermometers and other necessary equipment in order to transition to a South Korea type of testing, tracing, and quarantining of new cases.
I wonder if South Korea also had better tests?
” Did Our “Testing Fiasco” Really Matter Much In the End?
An ICU doctor writes to tell me that the problem with false negatives on the coronavirus test is worldwide:
‘ It’s been reported in the US, China, and Italy for a number of weeks that the sensitivity of the RT-PCR swab test for COVID-19 is not great. To put it simply, the issues aren’t specific to the US version(s) of the COVID-19 tests….We’ve known from very early on in the outbreak that the SARS-CoV-2 virus has higher affinity for receptors that are in the lower respiratory tract than it does for those in the NP/OP region like typical circulating coronaviruses. Given the dangers to healthcare workers of attaining lower respiratory specimens and the massively increased resources to do so safely, no country has moved to expectorated sputum samples outside of hospitalized patients, and even then only rarely.
This issue was obvious and widespread to Chinese and Italian authorities who have published numerous studies that predominantly used CT scans looking for a particular pattern of lung disease that most COVID-19 patients seem to demonstrate.
Not sure if that’s helpful or not, but this is something that physicians have rather widely understood for a number of weeks, but has not appeared to reach national leaders, which is sad.’
For the past couple of weeks I’ve been posting daily updates on the spread of COVID-19 in western countries, and one of the things that’s caught my attention is the fact that virtually every country seems to be on the same track. Some are farther along (Italy, Spain) and some still have a ways to go (France, USA), but the growth curve looks awfully similar in every case. But how can that be if every country has different testing regimens?
Without any explanation for this, I’ve been reluctant to speculate. But perhaps the explanation is the poor sensitivity of the COVID-19 PCR test? To put it bluntly, if the test is so bad that it misses a third of all cases, how much does testing even matter? I can even imagine that widespread testing might be detrimental if it produces a big pool of people who are infected with COVID-19 but feel confident that they aren’t.
An ICU doctor writes to tell me that the problem with false negatives on the coronavirus test is worldwide:
It’s been reported in the US, China, and Italy for a number of weeks that the sensitivity of the RT-PCR swab test for COVID-19 is not great. To put it simply, the issues aren’t specific to the US version(s) of the COVID-19 tests….We’ve known from very early on in the outbreak that the SARS-CoV-2 virus has higher affinity for receptors that are in the lower respiratory tract than it does for those in the NP/OP region like typical circulating coronaviruses. Given the dangers to healthcare workers of attaining lower respiratory specimens and the massively increased resources to do so safely, no country has moved to expectorated sputum samples outside of hospitalized patients, and even then only rarely.
This issue was obvious and widespread to Chinese and Italian authorities who have published numerous studies that predominantly used CT scans looking for a particular pattern of lung disease that most COVID-19 patients seem to demonstrate.
Not sure if that’s helpful or not, but this is something that physicians have rather widely understood for a number of weeks, but has not appeared to reach national leaders, which is sad.
For the past couple of weeks I’ve been posting daily updates on the spread of COVID-19 in western countries, and one of the things that’s caught my attention is the fact that virtually every country seems to be on the same track. Some are farther along (Italy, Spain) and some still have a ways to go (France, USA), but the growth curve looks awfully similar in every case. But how can that be if every country has different testing regimens?
Without any explanation for this, I’ve been reluctant to speculate. But perhaps the explanation is the poor sensitivity of the COVID-19 PCR test? To put it bluntly, if the test is so bad that it misses a third of all cases, how much does testing even matter? I can even imagine that widespread testing might be detrimental if it produces a big pool of people who are infected with COVID-19 but feel confident that they aren’t.
If this is the case, it would also mean that the testing fiasco in the United States didn’t really have much effect. We didn’t “squander” two or three weeks of time. In the end, it hardly mattered at all.
For now, consider this speculation. But I would sure like to hear from some experts about it.”
https://www.motherjones.com/kevin-drum/2020/04/did-our-testing-fiasco-really-matter-much-in-the-end/
EM:
Read NDd, who has stated repeatedly the US is not testing enough to get ahead of the curve. As a result the lockdown will take far longer. On the numbers, NDd is far ahead of the shit-stirring Kevin Drum who displays a lack of knowledge and is read for his prominence and not for his knowledge.
Testing does matter.
It matters when one becomes ill, the people who have been contacted by the ill person must also be tested, subsequently isolated 14 days if not showing symptoms to make sure, and those who are showing symptoms are treated and isolated. The tests should be done twice to confirm results. The US is not testing enough or isolating people, is testing at 5:1, while South Korea was testing and still is testing 15:1 and following through on the isolation routine. The US WILL NEVER get ahead of the curve and we will be locked into lockdown for monthS. Furthermore, the “don’t tread on me” states such as Florida (who finally locked down), Nebraska, Wyoming, etc. actions guarantee we will live with this virus much longer because they will not be told.
The R-naught for Corona is “thought” to be ~2.5 or for every person infected there is the possibility they will infect 2 and 1/2 others. Hence the need for more testing to capture those others. We need more testing to also firm the ~2.5 number up and also to determine CFR or the deaths resulting from Corona. It is strange how the Koreans can get ahead of the curve and we find excuses to dismiss testing in spite of limitations.
I’m not disagreeing with NDD at all on this topic. Just pointing out that it appears the success rate of some of these tests is horrible. And a false negative is a huge problem as that person moves on down the road.
And Drum does say his post was speculation.
EM:
The Koreans lived through it; but then, they are Koreans and we are Americans. Adapt, improvise, and Overcome. We make too many excuses. Just read Marshall’s post on NC. Labor is cited again as problematic to manufacturing costs.
More excuses.
I have not read NC since Yves censored me for calling out a lie about Obamacare written by one of her friends.
It was a guy living in Florida (I think) who stated his bronze plan cost him x amount of dollars to cover him, his wife and his family. I got him to give me his income and zip code and showed him a bunch of plans that were way, way less.
I’m sure you remember all of the attacks on the ACA for what is wasn’t on NC. And of course the blame went to Obama and Pelosi. Personally, I belive it was the attitude of normally progressive voters towards what the ACA wasn’t that caused the 2010 Mid term results. Sort of like the benriebros in 2016.
That is typical . . .