Rural Hospitals Closing Leaving Millions with No Hospital Care
Millions of Americans No Longer Have Hospital Care in Their Community
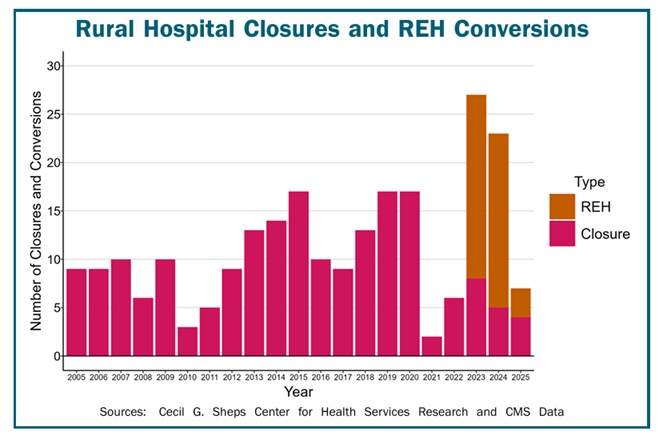
Over the past decade, more than 100 rural hospitals have closed. As a result, the millions of Americans who live in those communities no longer have access to an emergency room, in patient care, and many other hospital services that citizens in most of the rest of the country take for granted.
In addition, 40 hospitals have eliminated inpatient services since the beginning of 2023 in order to qualify for federal grants that are only available for Rural Emergency Hospitals (REHs). Every year, more than 7,000 rural residents had received inpatient care in those hospitals, but now seriously ill individuals in their communities will have to be transferred to a hospital far from home in order to receive the services they need.
Hundreds More Rural Hospitals Could Close in the Near Future
More than 700 rural hospitals– one-third of all rural hospitals in the country– are at risk of closing because of the serious financial problems they are experiencing. Over 300 of these rural hospitals are at immediate risk of closing because of the severity of their financial problems. (See Rural Hospitals.org for
the methodology used to estimate risk of closing.)
- Losses on Patient Services: Almost half of the rural hospitals in the country lose money delivering patient services. It costs more to deliver health care in small rural communities than in urban areas, and many health insurance plans do not pay enough to cover these costs.
- Insufficient Revenues from Other Sources to Offset Losses: Many hospitals have managed to remain open despite losses on patient services because they receive local tax revenues or government grants. However, there is no guarantee that these funds will continue to be available in the future or that they will be sufficient to cover higher costs. The special federal assistance many hospitals received during the pandemic has now ended. As a result, more than one third of rural hospitals lost money overall in 2023-24.
- Low Financial Reserves: The hospitals at greatest risk of closing have more debts than assets, or they do not have adequate net assets (i.e., assets other than buildings & equipment, minus debt) to offset their losses on patient services for more than a few years.
Rural hospitals are at risk of closing in almost every state. In the majority of states, over 25% of rural hospitals are at risk of closing, and in 11 states, 50% or more are at risk.

Rural Hospital Closures Harm Patients and the Nation’s Economy
Most at-risk hospitals are in isolated rural communities, where closure of the hospital would force residents of the community to travel a long distance for emergency or inpatient care. Moreover, in many cases, the hospital is the only place where residents can get laboratory tests or imaging studies, and it may be the principal source of primary care in the community. As a result, closure of the hospital would cause a loss of access to many essential healthcare services. In addition, rural hospital closures threaten the nation’s food supply and energy production, because farms, ranches, mines, drilling sites, wind farms, and solar energy facilities are located primarily in rural areas, and they will not be able to attract and retain workers if health care isn’t available in the community.
Closures Are Caused by Inadequate Payments from Private Health Plans
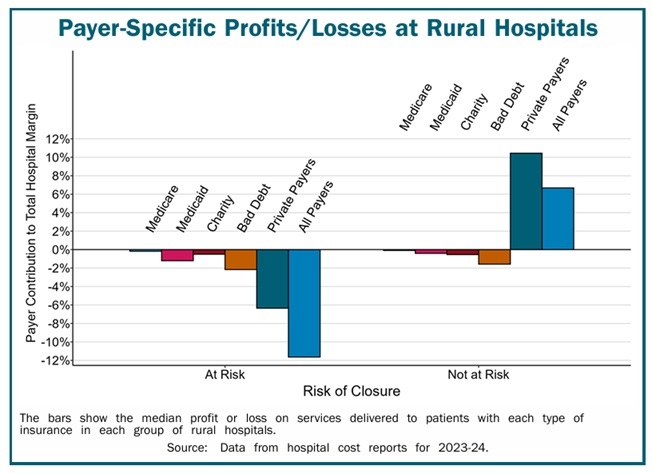
The primary reason hundreds of rural hospitals are at risk of closing is that private insurance plans are paying them less than what it costs to deliver services to patients. As shown below, although the at-risk hospitals are losing money on uninsured patients and Medicaid patients, losses on private insurance patients are the biggest cause of overall losses. Conversely, many other rural hospitals are not at risk of closing because they make profits on patient services. They receive payments from private health plans that not only cover the costs of delivering services to the patients with private insurance, but those payments also offset the hospitals’ losses
on services delivered to uninsured and Medicaid patients.
Most “solutions” for rural hospitals have focused on increasing Medicare or Medicaid payments or expanding Medicaid eligibility due to a mistaken belief that most rural patients are insured by Medicare and Medicaid or are uninsured. In reality, about half of the services at the average rural hospital are delivered to patients with private insurance (both employer-sponsored insurance and Medicare Advantage plans). In most cases, the
amounts these private plans pay, not Medicare or Medicaid payments, determine whether a rural hospital loses money.
How to Prevent Rural Hospital Closures
Private insurance companies and public insurance programs need to make significant changes in both the amounts and methods they use to pay for rural hospital services in order to prevent more rural hospitals from closing in the future.
Require That Health Insurance Payments Cover the Cost of Services in Rural Communities
Payments that are sufficient to cover the cost of services at large hospitals will not be adequate at small rural hospitals because it costs more to deliver healthcare services in rural communities. This is not because rural hospitals are inefficient, but because of the smaller number of patients served relative to the fixed costs of the services. For example, a small rural community will have fewer Emergency Department (ED) visits than a larger community simply because there are fewer residents, but the minimum cost of staffing the ED on a 24/7 basis will be the same, so the average cost per visit will be higher.
Congress should require that Medicare Advantage (MA) plans pay small rural hospitals adequately. MA plans should pay at least as much as Original Medicare pays for the same services,
and plans should be required to pay claims in a timely fashion.
Employers and residents in rural communities should choose private insurance plans that pay their hospitals adequately. Most private insurance plans are unlikely to increase or change their payments unless businesses, local governments, and residents choose health plans based on whether they pay enough to sustain local healthcare services.
Rural hospitals should not be forced to eliminate inpatient care in order to receive higher payments for other services, as is required under the federal “Rural Emergency Hospital” program. Federal programs should preserve and expand rural healthcare services, not reduce them.
Increasing payments to levels sufficient to prevent closures of the at-risk hospitals would cost about $6 billion per year 1/10 of 1% of total national healthcare spending. Most of the higher spending would support primary care and emergency care, since these are the biggest causes of losses at most small rural hospitals. Spending would likely increase as much or more if hospitals close, because reduced access to preventive care and failure to receive prompt treatment will cause rural residents to be sicker and need more services in the future.
Create Standby Capacity Payments to Support the Fixed Costs of Essential Rural Services
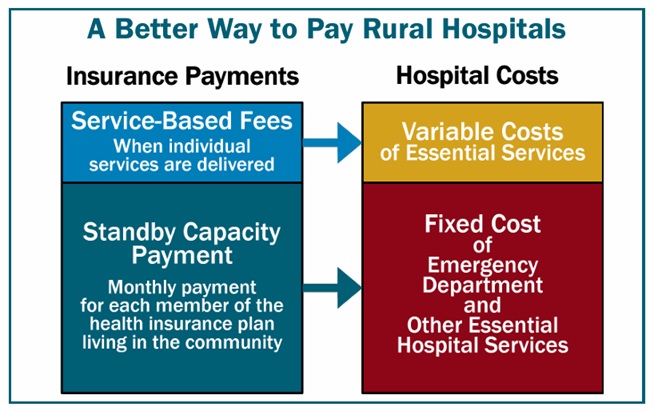
The financial problems at small rural hospitals are caused not only by the inadequate amounts paid by insurance plans, but by the problematic method all payers use to pay for services. The hospitals are paid nothing at all for one of the most important services for a rural community– having physicians and nurses standing by to treat an injury or serious health problem quickly. Having health insurance that pays fees when injuries or problems occur is of little value if there is no Emergency Department or inpatient care available for the resident to use.
in rural communities, small rural hospitals need to receive Standby Capacity Payments from both private and public payers in addition to being paid Service-Based Fees when individual services are delivered. The Standby Capacity Payment would support the fixed costs of essential services at the hospital, and the Service – Based Fees would cover the variable costs of those services. More details on this approach are available in A Better Way to Pay Rural Hospitals.
“Rural_Hospitals_at_Risk_of_Closing,” CHQPF
Great Post! You identify the problem which most people know about, but go beyond that to drill down to the actual causes as well as possible solutions. Now the question is where will the political will to address the problem come from? Certainly, not from the GOP which is dominant in rural areas, but I am not hearing anything from the Democrats other than wailing about Medicaid cuts. Those cuts will exacerbate the problem (after the 2026 midterms) but per your post is not the source of the problem as it exists today. That problem is the whole concept of health insurance.
Terrance:
I will take credit for presenting the topic here. However, this is 95% a CHQPR document that I am able to copy and paste here at Angry Bear. They identified the issues and I brought it to Angry Bear. Thank you for the read and comment!
Bill
Terry:
Rural hospitals are less likely to have funding which would typically come from local governments. Medicare, and Medicaid. Being smaller, their overhead is still high in comparison. Just like a small business.
The next issue being what type of resources should they have? Should they have XRay units which stand idle much of the time? XRay staffing their 24 hours a day? Logistics comes into play.
@Bill,
Also, hospitals are required to treat emergencies, even if the patient cannot pay. The hospital has to eat the cost. Smaller hospitals are already struggling, and converting Medicaid patients to indigents will increase that strain.
Thank you, Joel,:
I was attempting to explain why Rural facilities are having issuss in staying open and having the necessary resources. You just added to my reasons. An important reason at that.
@Bill,
Tragically, this all happens after the midterms. No accountability.
Joel:
People do not learn. Doomed to repeat the same mistakes over and over,